
Pamela Wible, M.D., takes on physician suicide in her TEDMED talk (delivered on November 18, 2015 and now released to the public on March 23, 2016). Learn more about Dr. Wible and her talk at TEDMED.com. Full transcription below:
I love the three things that people fear the most: death, disease, and public speaking. Here’s how it all started. At four, I was so talkative (and bossy) no babysitter would stay with me. So I tagged along with Mom, a hospital psychiatrist, interviewing suicidal patients. Then she’d drop me off at the morgue with Dad, a pathologist. He’d open these big cooler doors and say, “Good morning! Is anyone home?” then introduce me to his patients as a “doctor in training” and leave me there talking. My first captive audience!
Now I’m a doctor and I’m speaking on behalf of thousands of doctors who couldn’t be with us. But they’re here in spirit. I simply ask that you open your heart to their words . . .
“Dear Momma and Daddy, I know you may not understand why I didn’t seek help, but this choice makes sense to me. I know I would have been such a successful doctor and wife and mother. I love you so much, Your daughter, Kaitlyn.” Date of death: April 11, 2013. Cause of death: asphyxiation by helium inhalation due to untreated depression in medical school.
Each year more than one million Americans lose their doctors to suicide.
Across the country, our doctors are jumping from hospital rooftops, overdosing in call rooms, found hanging in hospital chapels. It’s medicine’s dirty secret. And it’s covered up by our hospitals, clinics, and medical schools.
No medical school wants to be known as the suicide school. No hospital wants to be #1 for interns jumping from rooftops. No one wants to become a doctor—to kill themselves. It’s the ultimate oxymoron: the barefoot shoemaker, the starving chef, the suicidal doctor.
So why? What the hell is going on? And why is this such a secret? And why am I piecing this together between patients? I’m a solo family doc, yet somehow I’ve become an investigative reporter, a specialist in physician suicide. Why? Mostly because I can’t stop asking why. Why both doctors I dated in med school died by suicide. Why eight doctors killed themselves—just in my sweet little town. So I keep talking and writing—and listening for the truth. And because I’m listening with my heart and soul 24/7, my cell phone has turned into a suicide hotline and I’ve received hundreds of letters from suicidal physicians.
You may be wondering: why do so many people “who want to help people” kill themselves?
Anna, a retired surgeon writes, “Dear Pamela, I was happy, secure, and mostly unafraid until med school. I recall in vivid detail the first orientation day. Our anatomy professor stood before an auditorium filled with 125 eager, nervous, idealistic would-be healers and said these words: ‘If you decide to commit suicide, do it right so you do not become a burden to society.’ He then described in anatomical detail how to commit suicide.”
What better way to bring shame to your alma mater than with a failed suicide. Alma mater means “kind mother,” yet doctors describe med school as “a soul-crushing boot camp, a dehumanizing nightmare, my own personal Vietnam.” Medical training is neither motherly nor kind.
“I love you mom. I’m sorry. Vincent.” Date of death: August 25, 1998. Cause of death: asphyxiation by hanging due to bullying, hazing, and sleep deprivation as an intern at a New York hospital.
Sleep deprivation is a torture technique. Fear as a teaching tool just teaches us to be afraid. I can help doctors, though there’s one group I can’t help—patients. From all over the country they write me, begging me to find them caring doctors. How can we give them the care we’ve never received?
“Dear Pamela, I definitely graduated med school with PTSD. It has changed me forever. I will never be the same again. We had two suicides and one murder, skull crushed with a bat, and another serving life in prison for murdering a classmate during a delusional episode after not sleeping for a month. Please change medical education. We were so beaten down. It takes a lot for me to cry but I cried all the time along with everyone else, but we hid it from each other, of course.”
Fact: we enter medicine with our mental health on par with or better than our peers. Suicide is an occupational hazard of our profession.
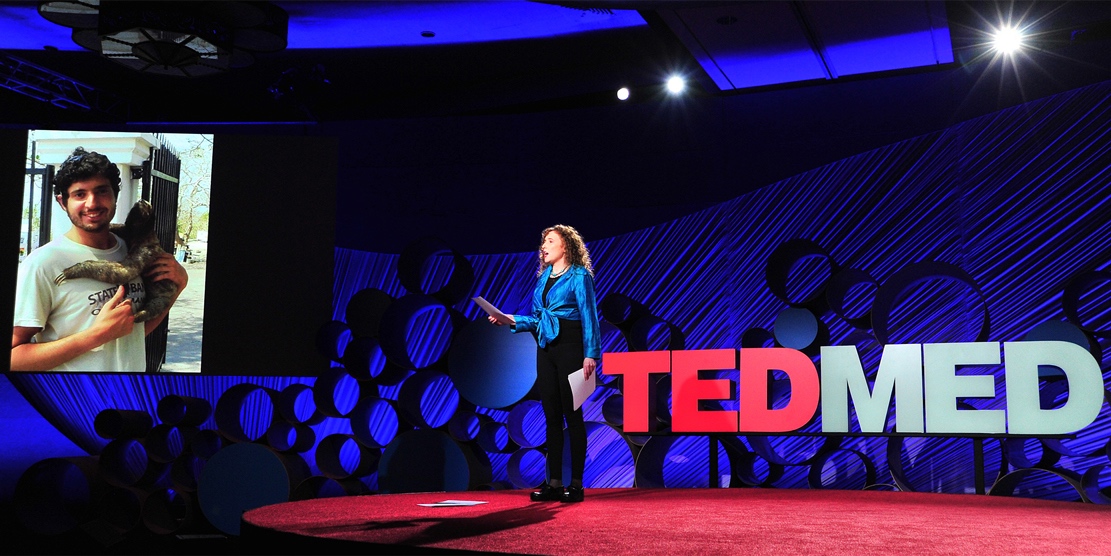
Photo credit Jerod Harris for TEDMED
“Dear Some, My family, I love you. To others who have been good friends, I love you too. This is just the end of the line for my particular train. Earth wasn’t a great place for me. We’ll see what else is out there. Will miss you all! I’m sorry for what it’s worth. Love Greg.” Date of death: June 22, 2012. Cause of death: Hemorrhage by transection of the arteries to his wrists and ankles. Okay so what happened here? Greg died just hours after being told not to follow his psychiatrist’s safety plan. By whom? By an agency (with no physician oversight) that controlled his medical license.
Our medical schools, clinics, hospitals (and related “agencies”) actually cause mental health conditions in doctors, then they blame us and force us to release our confidential medical records. And in the end, they take our license. But it gets worse . . .
“Dear Pamela, Do you know what really hurts? The fact that anyone can look me up on the Internet and read my dirty laundry. I’m publicly shamed, punished for being ill. I will only know peace when I am gone.”
Maybe that’s why my friend, an excellent psychiatrist, drives 200 miles out of town, pays cash, and uses a fake name to get mental health care.
“Dear Pamela, You don’t know how thankful I am for your article on physician suicide. I wanted to hug you after reading it. I had a really rough day—130 outpatients, sixty emergency admissions in a twelve-hour shift. I’m a final year internal medicine resident in one of the busiest hospital in India. Two patients on each bed, two lying together on the floor. Poverty, misery, pain all around. I’ve declared twelve patients dead in a day. I just don’t feel death anymore, just don’t feel human. My uncle died recently, I felt nothing. This profession demands too much from us. I’ve thought of suicide a thousand times. The misery is too much for me. . .”
I’m a perpetual optimist, yet after a decade of seven-minute visits at assembly-line clinics, even I felt suicidal. I thought I was the only one.
Then I got this crazy idea. What if I ask for help? Not from the profession that wounded me. So I asked patients: “What is ideal health care? What kind of doctor do you want?” They told me an ideal doctor is happy, has a big heart and a great love for people and service and an ideal clinic is a sanctuary, a safe place, a place of wisdom with fun flannel gowns, complimentary massage while waiting, where nobody is turned away for lack of money. I followed their instructions—and opened their ideal clinic—the first clinic designed entirely by patients!

Photo credit Sandy Huffaker for TEDMED
My life is like a lovefest now! My patients and I have inspired hundreds of doctors all across the country to open ideal clinics. At times I feel like the happiest doctor in America—until I get yet another call about a suicide or I read a letter like this:
“Dear Dr. Wible, I’m a patient who just got home from another insulting, degrading appointment with my doctor. I’m literally crying as I write to you. . .”
I call her. She shares her horror story. I share mine. She never knew doctors could be suicidal. She never knew she could be the victim in a cycle of abuse that began on day one of med school when her “insulting” doctor was still an idealistic student. How could she know that abused medical students become abused doctors who may one day abuse patients?
So how do we stop institutional abuse? Physician suicide hotlines inside our hospitals? Resilience training for our wiped-out doctors? Meditation classes for medical students? Wait, is our goal to help victims cope with abuse? Or to end the abuse?
It’s not costly or complicated to stop bullying, hazing, and abuse. It’s been outlawed from elementary schools to fraternities. Why not health care?
Medical culture and education must change. Yet cultures and institutions don’t change because we ask them to change—even when it’s in their self-interest. They change when they’re forced to change.
I favor the honor system. What if those in charge are not behaving honorably? What if our medical system continues to blame, shame, and publicly humiliate its victims?
Maybe it’s time for us to give them a dose of their own medicine. How? By shining an embarrassing public spotlight on physician suicide.
On behalf of those we’ve lost (and those who are barely hanging on), I want to thank you for shining your light into the darkness—because if we all shine our lights together, there’s is no darkness to fear. But mostly I want to thank you for your courage, for following a fearless little four-year-old through the morgue and into the coolers to meet a few of her friends.
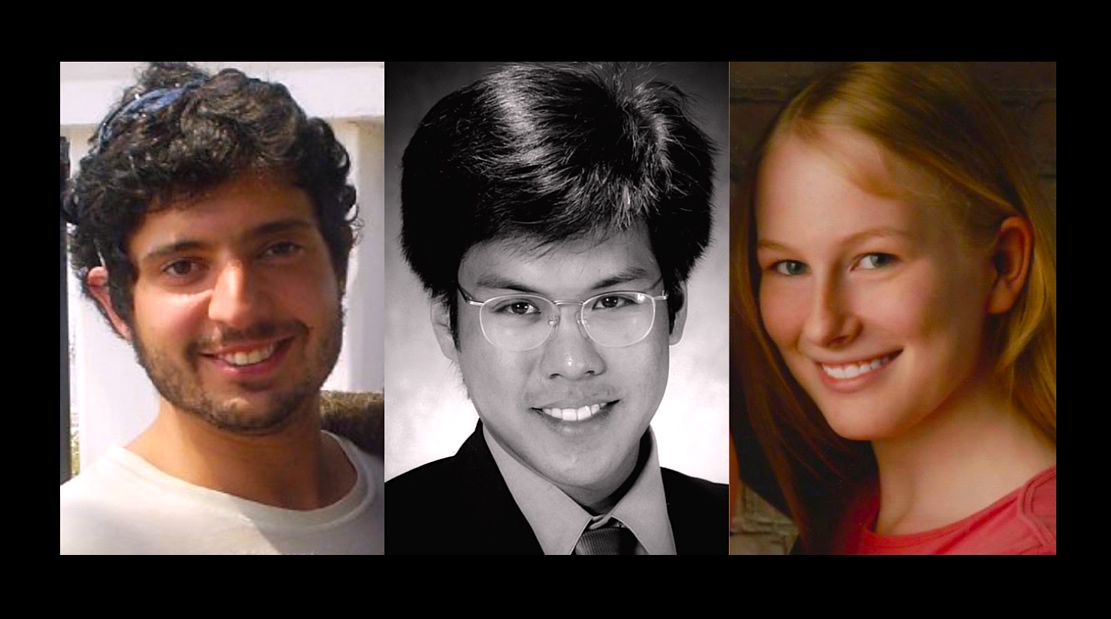
Greg Miday, Vincent Uybarreta, Kaitlyn Elkins ~ Rest in peace sweet souls. We miss you.














I’m for it! NOT in favor of teaching/training abused workers to tolerate their abuse. Let’s do the spotlight plan, and turn some shame and blame on institutions where high rates of suicide happen. I agree that no one wants to be known as the resident-suicide-place-to-match, and think it could be a big motivator to drop the macho-haven’t-gone-to the bathroom- in-17-hours pride in suffering and the cheapness that prevents adequate staffing. But I couldn’t help noticing that you named no institutions in your talk/transcript. I would certainly be fired if I did, and although you don’t have noticeable institutional ties, I sense that very bad things would happen to you if you did name names of other than the victims of abuse. Secrecy in the name of confidentiality just protects the abusers. I’d like to see some ideas about how to break through this Catch-22. Anybody?
Oh I know the names of institutions. For safety of the victims I did not share which hospitals, clinics, and medical schools were involved. I think we can all look around and see unhappy physicians, medical students, health workers, and patients in most every “health care” institution. This must change. How? We can’t solve a problem nobody knows exists. So . . .
1) Step 1 – Shine a spotlight (increase public awareness and decrease professional denial)
2) Step 2 – Allow institutions to autocorrect their inhumane practices
3) Step 3 – Force those institutions that do not comply with the United Nations Declaration of Human Rights to face severe penalties.
And yes these are human rights abuses in our hospitals, clinics, and medical schools. Meet one whistleblower here: https://www.idealmedicalcare.org/blog/physician-whistleblower-exposes-human-rights-abuse-in-u-s-hospitals/
I like this. Wrong is wrong, and abuse IS abuse! Doctors, medical students, health care students and providers, all are entitled to their human rights and humane treatment.
What other profession would allow 168-hour shifts and this level of abuse? https://www.idealmedicalcare.org/blog/physician-burnout-is-physician-abuse/ (watch these 3 short whistleblower videos)
Pam;
The comment in an earlier talk of yours about how we took care of soldiers with PTSD but if an abused health provider seeks help from the euphemistically-named “Physician Health Plan”, they’ll be reported to their respective medical board and yanked right out of practice. PHP’s are the worst! Boards are every bit as bad. I am an abused physician! I am not burned out. I’ve had my personal protected mental health information posted online by my medical board–it’s their policy, while the PHP stands by in tacit approval. After signing a PHP contract and doing everything it mandated, the level of advocacy I received was “just do whatever the Board tells you to do”!
This must change!
Please do not publish my name or EMail but DO publish my website!
I read your book. The system IS BROKEN.
We can fix it … together.
Stop the money at the schools… the source of the problem.
It will snowball in a short time this time gaining upwards momentum.
We can and will change this system.
Dr’s torture each other and they harm patients.
It drs don’t like each other … I got no chance.
The stories told in your book were heartbreaking. Stories of the victims made me so sad. It blew my mind how people are bullied by coworkers and how that changes their perspective of patients. It’s like a never ending circle of poor energy.
I also wonder to what part prescription medications play in this whole story.
The drugs that have the acceptable side effects of uncontrollable urges.
Maybe this info should be disclosed to patients… as it only rolls downhill to us. Doctors are at some point patients too.
Together we can make this system better. I was abused by these bullies as a patient and physically harmed. I have total proof… I hope someone will help me.
I will change this broken system of zero accountability… If YOU want me on your team I AM READY!
You’re not going to fix or change anything – other physicians are the leading cause of physician suicide whether in training or in practice. I’ve got plenty to tell you with histories of my Mayo Clinic trained dermatology wife and misdiagnosed Ehlers Danlos HM, severe narcolepsy, and pain issues along with my bad psoriatic arthritis/chronic pain for 23 years of my 30 in practice as a senior staff pathologists. The vast majority of pathologists don’t troll morgues BTW. After two decades of bad disease and great management with the dreaded opioid meds, the CDC and other addictionology malcontents are out to eliminate chronic pain care and it’s much better to be an addict these day rather than be people who play by the rules – we don’t count anymore. The deck is stacked against anyone who does things correctly and survives and state medical boards don’t care for physicians who are ill and on meds being monitored by other highly qualified physicians (even if they are very well liked with impeccable credentials). The fiasco we’ve endured would have killed many but we’re still here and I’m hoping to make others who’ve helped put us in this position as miserable as possible.
I started this journey with the conviction that God chooses his healers and brings us to the place where we get to learn medicine and learn to be his healing hands. We are honored to be chosen to interface with people in vulnerable times and be a conduit for God’s healing. I still believe that but I am a hell of a lot more jaded and grouchy about it than when I started. I agree that medical education is torture at times. Internships and residencies are very challenging. I was blessed beyond measure to attend the residency that I did and I KNOW many physicians are not as fortunate to get a good education in a supportive environment. This breaks my heart. I would like to bring up an additional stressor on the physician. The patient and the public. Our healthcare infrastructure is getting heavier and heavier with regulations and data gathering and medical/legal concerns and all of that funnels to the physician (at least to primary care). In the same breath that more and more has to be done by the physician and no longer by staff helpers, the demand for more people to be seen in a given day is increasing at a frightening rate. The logistical burden is overwhelming and we haven’t even begun to talk about the patient. We need to be focusing on sensitive caring personal interactions with a patient and they need to be HEARD and LOVED. But 40 of them want to be heard and loved all in the first HALF of the day. Patients do not consider physicians to be human. They believe we are machines who exist for their need to be met. They expect a level of customer service that they don’t demand from any other industry. And yes the patients experience its the whole reason we are in this gig but the bottom line is….. with only 24 hours in a day, physicians can give quantity or quality but not both. And if physicians are not allowed time to tend to their families and their health, with the support of their coworkers and other physicians, they will not be able to give quantity or quality but instead will throw in the towel and quit (or even worse as Dr. Wibel discusses above). I guess my point is, societal pressures on the physician machine, system wide pressures of tasks piled on increasing every day are just ways in which the flame the we start with quickly gets snuffed out and we loose our love for patients and our love for life. Finding the joy in practice has become my priority. I’ll take joy over a big paycheck any day and I want to work towards helping other physicians find joy again.
-MGN (primary care physician)
Yep. Physicians are viewed as servants, not people. We have the same wounds, scars, and we bleed and cry like everyone else. It’s just hidden under the white coat.
“We need to be focusing on sensitive caring personal interactions with a patient and they need to be HEARD and LOVED.”
It is unfortunate that the profit driven push by current primary care system has all but eliminated any kind of sustained personal interaction with the patient… It is impossible for conventional medical doctors to accurately assess complex medical issues in the minuscule amount of time they are given per patient. The fault lies in the lap of a broken system driven by profit rather than patient centered care. Sad but true…Many conventional docs are even opting out of the current system altogether in search of a “care model” that suits their needs as practitioners and respects the expertise it has taken them years to cultivate.
Thank you for an eye opening look at the other side of health care from the physicians perspective…Everyone is so hyper-focused on the physicians lack of empathy for their patients…This gives us all a much needed look behind the lab coat.
Exactly Cyndi. Giving a multiple choice test on empathy just before graduation will not put the empathy back in medical students. Let’s not injure them in the first place.
I attended a medical school which for the most part, treated it’s students as new colleagues. There were two notorious services in the hospital which were either avoided or sought out to prove one’s toughness. Interestingly, the students coming off those services were scarred. After match day they wore FYBIGMI badges: “Fuck You Buddy, I’ve Got My Internship.” The rest of us found those slightly embarrassing.
After nearly 40 years of teaching, I’ve had far too many chances to meet physicians who had survived the other tradition. Reinforcing the idea that medicine consists of Caring for people as an act of love became the theme which grew over time.
Keep up the writing. I’m more traditional, but still feel that survival requires living your values. I think the most soul-sucking factor at the moment is practicing to the EHR and the ICD-10. The happiest physicians I’ve seen are those who’ve opted out of that.
Take away the debt and most people will quit medicine. Every day I dream of the day of winning the lotto to just pay my loans and exit. Every resident I work with says the same thing. We hate medicine, we hate the hospital we hate the patients, we hate the administrators, we hate the hours, we hate the pay, we hate the paperwork, we hate every aspect of it. We talk about it daily. Wouldn’t do this again. We want out of this sh*t.
It is amazing, we sacrifice to take care of people who don’t care or want to take care of themselves while losing our own health, relationships, sanity, and diving deep into debt only to have them turn around and want to sue us. Ya, you wonder why doctors wanna kill themselves? I’m surprised more haven’t snapped yet.
Cannot remember the last time I smiled. Institutional abuse won’t stop. My residency makes us lie about our hours. Our GME dept sits us down has us log in and instructs us to change the hours to have no “hour violations” so they cane say nobody went over 80 hours. They make 1 intern cover 15 patients alone with no senior backup. The same Older Doctors who were crooks that stole from the medical system and abused it are the ones saying “interns and residents shouldn’t have work hour restrictions” so they could use us for free labor to make them money. These hospitals make money over fist with us.
It’s so f*@ked up. Call OSHA. Report your hospital to OSHA.
I have mentioned the solution and nobody even asked about it. So I am going to give the solution and explicit instructions how to solve the problem:
Any concerned citizen (you do NOT have to be an employee there) can contact the local OSHA office and alert OSHA about a potentially unsafe workplace. If there is a work-RELATED fatality, that triggers an automatic OSHA investigation.
If you are an employee there are whistleblower laws that protect your position. OSHA also covers interns, volunteers, and students in the workplace as well.
When there is a physician suicide in the news, call the local OSHA office as a concerned citizen about potentially unsafe working conditions that have lead to this. You can reference Pamela’s website and book (http://www.physiciansuicidelettersanswered.com) as proof the suicide is work related for physicians. Employers must (by law) report work-related fatalities to OSHA.
Here is a link to the OSHA standard on workplace violence (which includes bullying)
After just a couple OSHA investigations, watch the industry change.
Problem solved.
Do it Michael.
~ Pamela
A Banterings also states you can preserve your anonymity: “They can just send a letter anonymously (unsigned) to the local OSHA office stating that there is an imminent danger. You or anyone else can send a letter anonymously after a suicide asking OSHA to investigate claiming the suicide was work related.”
Thank you for bringing attention to this issue. My father came to the U.S. in 1970 to begin his medical career. From the beginning, he faced challenges. For one, he and his colleagues were barely paid anything (as residents, I believe), but were forbidden from moonlighting to make any extra money. Later, after I came along, he told me that I could be anything in the world I wanted to, except for a doctor, because it was a horrible life. Shortly after retiring he developed a rare blood condition and, instead of pursuing treatment, decided to take his own life. Reading your articles made me think about my father from a different perspective, and really feel sorry that he gave nearly five decades of his life to a profession, but then didn’t trust that profession to give anything back to him. The system is broken on all sides.
So sorry for your father’s suffering. Medicine has turned into a very cruel profession for so many physicians. Isolating. Lonely. Unforgiving. Dehumanizing. And the cycle of abuse continues unabated. Doctors are not allowed to be human beings. They are held to superhuman standards and those who stray from the norm are written up as “unprofessional.” Add uncontrolled capitalism to this mix and it is a very sad tale indeed for far too many.
Medicine does not have uncontrolled capitalism (an oxymoron) — the problem it does have in spades however is uncontrolled cronyism.
It’s professional cronyism by the medical fraternity that locks trainees out for non-valid reasons and keeps them stuck in their system. And it is societal cronyism (aka government in bed with corporations/professions “for the public good”) that creates the monopoly of the medical profession that can hide these abuses with the ultimate threat of kicking people out of their system.
True capitalism would be competition ie real choice all the way. Then doctors would leave and speak out without fear of losing all they had trained for, and employers would then have to make their workplace good enough to attract great workers.
Instead they can just bully and threaten, and back it all up with the power of government regulation and removal from the profession.
Excessive suicide rates is just one side-effect (unintended, but direct, consequence) of the NON-capitalist monopoly that is the medical profession. The incentives in a cronyist system mean that these problems can not be solved.
My personal method was to focus my energies on getting out of their control as much as possible. It won’t work for everyone, but the alternatives inside the system are often worse. Morfy below has the right idea.
So what are you doing now? Practicing?
Yes, I’m still working in medicine with patients. But I avoided trying to get into specialty training. Then I got lucky to find a lesser training program at a time when it didn’t have so much politics in it, so it only took a little bit of “lying” to be accepted and get through.
I’ve found a niche that doesn’t really use much of my medical training, but does give me an income as good or slightly better it seems than my peer colleagues, and with a better lifestyle for myself and my family.
On the way, I’ve dipped into other career and financial options such that if they took my license away now I would end up just shrugging my shoulders and moving on.
I’ve made mistakes, ducked as much bureaucracy/politics as I could, gone down dead ends, kept flexible financially, and had some lucky breaks.
But I think the key was that I knew what I wanted in life enough to put effort and time into finding, recognizing and taking alternative opportunities when they came up. Oh, and I had a partner who supported/tolerated me as I did all this — “but I thought I married a doctor!” she would say 😉
When I started medical school, I looked at the doctors that have been in 10–15 years as a guide: If I stay in medical school, THAT will be me in ~10 years. I didn’t like what I saw. You should also give yourself permission to bail, if the situation warrants. Sure, family & friends may be disappointed if you quit; compare that to how they’d feel if you killed yourself. They’ll get over you leaving medicine, they might even understand, eventually. Don’t let it ever get to the point where you’re contemplating suicide–bail. If a fighter pilot waits too long to eject (trying to save a multi-million dollar jet), they may not survive. Make a firm, positive decision, pull the handle, get the f*ck out! Take control of your life again.
600 people stand in solidarity to say “no more” medical student/physician suicides: