This summer I did the [ALS] ice bucket challenge. But I’m challenged by another disease. A disease so scary people won’t say it out loud. A disease so frightening that doctors are afraid to talk about it. A disease so feared that physicians falsify death certificates, families deny the cause of death, and most victims’ names are hidden for eternity.
Every year we lose over 400 doctors to suicide. That’s like an entire medical school—gone. I was suicidal. I survived. But I lost both men I dated in med school to suicide. And 3 doctors in my town in just over a year to suicide. Each year over 1 million Americans will lose their doctors to suicide. These are just the physician suicides I heard about this year:
Gregory Miday, MD, internist, by scalpel in bathtub
Vincent Uybarreta, MD, surgery intern, by belt hanging in closet
Kaitlyn Elkins, third-year medical student (and her grieving mother, Rhonda Elkins), both by helium overdose
David Brooks, MD, family doctor, by standing in front of train
Phillip Henderson, MD, III, fourth-generation obstetrician, by gunshot wound
Rafael, family doctor in South Carolina, by overdose
Gregg, internist in California, by overdose
Pediatrician in Oregon, by gunshot wound in park
Vascular surgeon in California, by carbon monoxide
Urologist in Oregon, by gunshot wound
Larry, anesthesiologist in Oregon, by overdose in hospital closet
Edward, family doctor in Oregon, by gunshot wound in clinic
Otolaryngologist in Kentucky, by jumping from balcony
Orthopedic surgeon in California
Anesthesiologist in Washington
Female third-year medical student in Michigan, by overdose
Another medical student in Michigan
Male surgeon
Male radiation oncologist
Male internist
Male doctor
Male doctor
Male colorectal surgeon in Texas
Male medical student
Male doctor
Male doctor
Male intern
Male pediatric surgeon, by gunshot wound in bedroom
Male doctor
Female internist
Male family medicine resident
Male doctor, by gunshot wound
Male family doctor, by drowning
Male second-year medical student in Washington, by gunshot wound
Male neurosurgeon
Cardiologist in California, by gunshot wound in laundry room
Male anesthesiologist
Female family physician in Iowa
Male anesthesiologist, by overdose in hospital
Another male anesthesiologist, by overdose in hospital
Male medical student
Jack, doctor
Male doctor in Oregon
Jose, doctor
Craig, doctor
Male physician
Male surgeon
Female physician
Female medical student
Another female medical student
Male medical student
Male doctor, by heroin overdose
Male pediatric intensivist, by plane crash
Male family physician, by gunshot wound
Female obstetrician, by driving off bridge
Male obstetrician, by gunshot wound
Male internist, by overdose
Male medical student, by jumping
Male medical student, by gunshot wound
Male physician
Male surgeon
Male family physician in Alabama, by gunshot wound in driveway
A married physician couple, by overdose
Another married physician couple, by overdose in hotel room
Female doctor in Wyoming
Male allergist in Oregon, by jumping from hospital parking garage
Rudolph Fajardo, MD, pediatrician, by gunshot wound
Bruce Feldman, MD, surgeon, by jumping from bridge
Male doctor
Captain Michael Ryan McCaddon, MD, Army obstetrician, killed himself at Tripler Army Medical Center in Honolulu
Nicholas DePizzo, MD, family doctor, by gunshot wound in office
Henry Norrid, DO, by gunshot wound
Male radiation oncologist in Illinois, by jumping from window
Leonard Graff, MD, by gunshot wound in clinic
Jonathan Drummond-Webb, MD, pediatric heart surgeon, by overdose
Harry Reiss, MD, urologist in NYC, by overdose in clinic
Male doctor
Carrie Largent, second-year medical student
Douglas Meyer, MD, gastroenterologist, by jumping from hospital window in NYC
Daniel Gunther, MD, pediatric endocrinologist, by inhaling car exhaust
Hamza Brimah, MD internist, by gunshot wound
Male doctor, by overdose
Male doctor, by gunshot wound
Female anesthesiologist
Medical student in Boston
Another medical student in Boston
A third medical student in Boston
A fourth medical student in Boston
Male otolaryngologist, by hanging himself in hotel room
Male anesthesiologist, by overdose at the hospital
Male family doctor, by gunshot wound
Male doctor, by gunshot wound
Male pediatric endocrinologist, by hanging
Male physician
Another physician
Medical student
Male physician
Male medical student
Male physician
Male physician in Oregon, by gunshot wound
Male obstetrician, by gunshot wound
Male family medicine resident, by gunshot wound
Male obstetrician, by gunshot wound
Female physician, by overdose
Male family physician, by overdose
Male obstetrician, by overdose
Male psychiatrist, by gunshot wound
Female medical student, by gunshot wound after failing exam by 2 points
Female pediatrician
Emergency room physician in Oregon
Female anesthesiologist, by overdose
Orthopedic surgeon in Seattle, by gunshot wound in car
Male physician, by jumping from hospital
Another male physician, by jumping from hospital
Pediatric cardiologist
Pediatric immunologist
Male urologist, by stabbing himself in abdomen in hospital parking garage
Female medical student
Female otolaryngologist, by carbon monoxide
Medical student
Surgeon in Houston, by gunshot wound
Male medical student
Male urologist in Oregon
Urology resident in Portland, by walking in front of a truck on highway
Female physician, suicided after not getting a dermatology residency
Last week I delivered this talk twice at the American Academy of Family Physicians Scientific Assembly in Washington DC, and I also presented it to third-year medical students at The Commonwealth Medical College of Pennsylvania. It is fully transcribed here. Every medical student and physician needs this information. Please share widely. You may save a life. Dr. Wible: Welcome to Physician Suicide 101: Secrets, Lies & Solutions.
I’m a family physician born into a family of physicians. My parents warned me not to pursue medicine. So I went to medical school. Ten years later, I’m unhappy with the direction of my profession (and I’m not the only one). Then I get this crazy idea: what if I ask for help? Not from the profession that wounded me. Just from random people on the street. So I hold a town meeting and ask patients to help me—design an ideal medical clinic. I promise do whatever they want as long as it’s basically legal. That’s going out on a limb.
I’m a go-out-on-a-limb kind of doctor. In med school I protest the dog labs and I’m sent to the office of the Dean—who diagnoses me with “Bambi Syndrome.” In residency I’m caught giving patients recipes for kale salad. I’m sent to the office, reprimanded for not getting approval from the patient education committee. I’m 46 and I’m still handing out unapproved kale salad recipes—now I’m taking on physician suicide. My therapist calls me the “Dr. Kevorkian of Medical Taboos.” Before my wedding, my dad actually made my husband promise to keep me out of jail. “Always pushing the limits,” Mom says, “always going out on a limb.” Today I invite you to join me.
Here are the official learning objectives. Bottom line—I need you to take action. I don’t care what you do as long as you do something.
Why do we do what we do? To save lives. Why did you go to medical school? Seriously. Why spend your 20s studying while all your friends are at parties? To make a difference—to save lives. Why are you here? To get CME? See the Smithsonian? Rediscover your joy, your calling? What is your calling? Why are you a family doc? They recruited me for pediatrics, but I kept asking why? Why this kid’s got asthma? Why the parents smoke? Why they live next to an incinerator? I’m a family doc because I can’t stop asking WHY? So why are you here? You had 20 choices, why attend this talk? Maybe you lost a colleague to suicide, a friend in med school. Maybe you are struggling now. Maybe (like me) you just want to know why our colleagues die by suicide at twice the rate of their patients. And you want to save lives.
The fact is each year we lose over 400 doctors to suicide—that’s like an entire medical school gone. I lost both men I dated in med school to suicide. In my town, in just over a year, we lost 3 doctors to suicide. One doc in town lost 7 colleagues to suicide! (In what other profession, can you lose 7 colleagues to suicide?!) This year over 1 million Americans will lose their doctors to suicide. Why? To know why someone has died, we perform an autopsy. With suicides, we perform a psychological autopsy:
Today—for the first time—I share my results from 4 psychological autopsies:
This is Vincent. He’s 2. He framed this photo to give his parents at his med school graduation. An adored first grandchild, a joyful little prankster who made everyone laugh. His Aunt Edna told me in catholic grammar school Vincent has his feet up on the chair in front of him. Sister Agnes comes by and tells him to put his feet down. He replies, “I have to keep my legs up!” She asks why. He says, “I have varicose veins.”
Here’s Vincent at high school prom. An athlete and artist, compassionate, sensitive, gregarious, yet private. A compulsive perfectionist. Always a good kid. Never any addictions. Just a straight forward normal good guy, according to his mom.
Here’s Vincent’s med school graduation photo—just 25 years old and 2 months after starting a prestigious surgical residency in New York City, he dies by suicide. Why? Look at his eyes. Notice the difference between his childhood photos and his medical school graduation picture. He looked happy and healthy before med school. What happened during Vincent’s medical training? I interviewed several of Vincent’s family members to find out.
His mom says he became disappointed, disillusioned. He lived near the hospital, but drove an extra 45 minutes home at every chance he had just to sleep in his own bedroom. He lost a lot of weight and his jokes and laughs were gone. His family was concerned, but they thought it was the adjustment to a demanding profession.
Vincent told stories of how surgeons publicly humiliated interns. How he and his partner fell asleep leaning against walls in the hospital while waiting for their patient’s turn for a scan. He spoke of his doubts about saving this one guy who jumped out of a building when caught raping a young girl who was also being treated in an adjacent room. He spoke of the sisters—victims of a car accident—brought to the ER, stunned him for a moment because they looked like his mom and aunt who often travel together without seat belts. Vincent took a belt and hung himself in his closet. The note he left:
* * *
This is Greg at 3.
Outgoing, curious and clever. He always got along great with adults. At 5, he goes on this family trip to visit his great aunt—a nun at a convent. A French professor, she asks Greg to give her a word he would like to hear in French. He says, “Guacamole.”
Greg as a child with his mom.
Greg graduating from med school. A pianist, painter, poet, a real Renaissance man much beloved by his patients. Greg sent this e-mail to his parents, both physicians, one year before he died
Subject: Piece of My Mind Read this if you have time. It resonated with me especially well this morning. I like these two paragraphs: I love practicing medicine. Unequivocally. Yet it sometimes seems as much a burden as a privilege. We begin our careers in the anatomy room, a ghoulish lab in which many ‘civilians’ would faint. We cut our teeth in bloody operating rooms and intensive care units from which few people leave intact. We spend our lives bearing witness to the sufferings and diseases of troubled souls. We are well paid, intellectually stimulated, and, if we are lucky, trusted and maybe even loved by our patients. Yet on certain days, when our patients do not do well, the trade-off seems untenable. How are we to protect ourselves from the emotional hazards of the practice of medicine? How are we to stand with our patients through the very worst while avoiding depression, significant stress reactions, and even substance abuse or addiction? Love, Greg
Greg was the only one in his family who struggled with anxiety, depression, and alcohol. After an outpatient program his third year of med school, he was sober until his second year of residency. A brilliant clinician, never impaired at work, but a Physicians Health Program (PHP) mandated a 90-day treatment facility 300 miles away, where Greg felt marginalized, belittled and was 3 months behind in completing residency. He felt if he were a banker or lawyer he wouldn’t have this forced upon him. He hid his depression and substance abuse and carried a lot of shame. Just 24 hours before his death (he had relapsed), he met with his psychiatrist who arranged admission at a local rehab facility. Greg notified the PHP who held the keys to his license. They disagreed with his psychiatrist’s safety plan. Greg felt humiliated, cornered, and killed himself. His mom wrote this letter to the editor of The New York Times in response to a physician suicide article last month. You may recall the article about the two young doctors—interns who jumped to their deaths in late August from their Manhattan hospitals. Greg’s mother writes:
An unacknowledged predicament for physicians who identify their struggle with substance abuse and/or depression is that they are often placed under the supervision of their State Medical Board’s Physicians Health Program. My son, Greg, was being monitored by such a program. He took his own life at age 29, one week before he was to enter an esteemed oncology fellowship. His final phone calls were to the PHP notifying them of his use of alcohol while on vacation, a disclosure he had previously described as a ‘career killer.’ These programs, which often offer no psychiatric oversight, serve as both treating and policing agencies, a serious conflict of interest. Threatened loss of licensure deters vulnerable physicians from seeking help, and may even trigger a suicidal crisis. Medical Boards have the duty to safeguard the public, but the assumption that mental illness equals medical incompetence is an archaic notion. Medical Boards must stop participating in the stigmatization of mental illness. We cannot afford to lose another physician to shame.
I read 12 pages of online condolences. This anonymous entry stands out: “Thank you for being nice to even the unpopular kids in high school. May your soul rest in eternal peace.” Greg looked out for the underdogs, but what happens when doctors are considered underdogs? Who looks out for us? Do we get the care we need? Greg didn’t. Greg transected his bilateral radial and dorsalis pedis arteries with a scalpel in the bathtub, candles lit, music playing, some wine, vodka, surrounded by family photos. Greg’s note:
* * *
This is Kaitlyn and her mom.
A sweet, good girl. Kaitlyn never gave her parents any problems, though she cried when she lost at Monopoly. From the time she started preschool, she never needed any help with her homework or anything. At 3 years old, she had to get glasses. Her parents took her to the big medical center where the doctor asked lots of questions. He’d look at the parents for answers, but Kaitlyn answered them all. The doctor was amazed.
This is Kaitlyn in high school. A deep thinker, an artist, a poet. I met her extended family in North Carolina. They claim, “Kaitlyn was one of the happiest people on this Earth.”
Here’s Kaitlyn in med school. Just 23 years old and beginning her third year. An introvert with social anxiety, Kaitlyn always had a few close friends, but none in med school. Everyone was busy studying and “people just went their own way,” she told her mom. She was desperately lonely. Her perfectionism worsened. She went on a strict diet, started running marathons, and lost a lot of weight. She ran like 10-12 miles before class everyday and still excelled in med school, acing her Step One exam. Unfortunately she didn’t live to celebrate her results because she completed her suicide—a helium overdose—like a well-planned school project. She left a 2-page suicide note in which she claimed lifelong depression, but hid it to protect her family and herself.
As an aside, I believe that Kaitlyn suffered less from depression and more from “feeling different and isolated” due to her high intellect. She was raised in the poorest county in North Carolina was the smartest person around. Maybe she had hoped that when she entered medical school she would finally be with her tribe—a social circle of more like-minded intellectuals. But medical school rarely creates an environment for students to develop intimate friendships with one another. These young sensitive and brilliant people are left to fend for themselves in survival mode with an overwhelming amount of material to master in a short time with little emotional support. I can guarantee that many medical students cry themselves to sleep at night in their pillows. That’s what I did nearly every night my first year of medical school. I cried so much that one morning my eyelids were sealed shut. I couldn’t see anything when I woke up. I had to feel my way to the bathroom. Is this they way a civilized society trains its healers? Kaitlyn’s mother published her daughter’s suicide letter in a book she wrote about Kaitlyn. An excerpt:
Kaitlyn’s grieving mother—unable to recover from her daughter’s death—died by helium overdose one year later. I attended her funeral last month.
* * *
Here we have a spunky, happy 2-year-old girl who stood up to adults negotiating her way out of a bedtime, a bath time, and persuading her dad to get Slurpees and candy bars for dinner. Life was good until her first year of medical school.
Just a few months into med school she develops major depression due to what she calls “barbaric and inhumane medical training.” Years later, fed up with assembly-line medicine, she’s suicidal. The only difference between these cases is she survived and she’s on stage speaking today for the other 3 who can’t.
* * *
Our cases are not isolated. All brilliant, sensitive people who felt alone in a highly competitive and inhumane environment. All sleep deprived working or studying over 80 hours week. All hid their depression and appeared highly functional until their suicides and all left notes because we’re trained to do and we’re so darn responsible!
The secrets start with victims who are ashamed. Families remain silent to safeguard their reputations. Physicians hide suicides from patients who never find out why they can’t get a follow-up appointment with their doctor who left the clinic so suddenly. Physician suicide is medicine’s darkest secret and our code of silence is maintained by layers of lies.
Reductionism is the opposite of holism. Reductionism leads to body-mind-spirit disintegration. While reductionist medicine has led to scientific advances, it’s fatally flawed. It separates us from our hearts and souls which is what gives our lives meaning and keeps up wanting to live here on Earth. Professional distance is far from protective. Vulnerability is strength. When we’re authentic with our patients and ourselves, we build resilience and connections with other people here on Earth. And the suicide coverups . . .
It’s a medical game of truths and lies. Death certificates are miscoded even when there’s a suicide note! A suicidal hanging becomes asphyxia, a suicidal overdose is suddenly an accidental overdose, a self-inflicted gunshot wound is officially an accidental gunshot wound, a suicidal motor vehicle accident is just another motor vehicle accident.
Meanwhile those in the know whisper blame-the-victim questions: Was he not doing well academically? Did she got a low board score? Are we selecting the wrong people for medical school? These questions focus blame on the victim, not the health care system.
So what are the solutions? Solutions come from individuals or institutions inside or outside of medicine.
Non-medical individuals—the general population of non-physicians. Except for Greg’s parents who are aware of the occupational hazards of medicine, families had no idea their child was at high risk of suicide until the police called to tell them their child was dead. Compelled to act, Vincent’s mom starts a foundation that sponsors an annual lecture on mental health for residents at Vincent’s school. Kaitlyn’s mom writes her heart out online in a blog and on social media sites. She supports struggling medical students online. Ultimately she publishes a book examining suicides in the exceptionally gifted like her daughter. She asks all 171 medical schools in the United States if they would like a copy. Thirty got a copy. Should we rely on grieving mothers—suffering in isolation as were their children—to solve this?
Non-medical institutions like the media could instantly stop the secrecy and alert the public about the high risk of suicide in medical students and physicians. Because sending your child to medical school or a surgery residency is not like sending your kid to law school or to cashier at Walmart. It’s more like sending your kid to Iraq or Afghanistan and it requires a completely different level of vigilance. I spent two hours on the phone with Kaitlyn’s dad the other week. A sweet, sweet man. Not the kind of guy who would ever blame anyone else for his problems. I asked, “If Kaitlyn worked at Walmart, would she and your wife still be alive?” He says, “Yes. Medical school has cost me half my family.”
Medical individuals—that’s me and you questioning these deaths, and Greg’s mom seeking audits of PHPs for fraud and abuse.
Lastly medical institutions. Kaitlyn’s school started a fund in her name for donations to their wellness center so that presumably Kaitlyn’s classmates could seek the help that she didn’t. Vincent’s yearly lectures continue. But what else can we do?
Let’s compare how we handle physician suicide with say. . . umm . . . human rabies. Since the 1900s, annual human rabies deaths in the US have gone from 100 to just 2 per year. How did we do this? Not by grieving mothers launching “rabies awareness campaigns.” Not by donations to a wellness program. Not by a yearly lecture series. And not by miscoding rabies deaths as the flu!
Here’s how we did it: medical institutions took this on methodically using science—primary, secondary and tertiary prevention strategies.
We spend over $300 million annually to prevent human rabies. The cost per human life saved ranges from $10,000 to $100 million. What do we spend on medical student and physician suicide prevention?
Since eradicating the terrestrial canine rabies variant in the US, 90% of the 2 deaths per year are transmitted from wildlife—mostly bats then raccoons. If we can deliver over 6 million oral rabies vaccine baits yearly to raccoons (and I’m talking about guys dropping these from low-flying planes over the Appalachian Mountains and dudes running through dark urban alleys), we’ve gotta be able to do something for med students. Right? We’re way easier to find than raccoons. We’re already in the hospital!
Right now while I’m standing here on stage we are actively tracking rabies in raccoons, bats, skunks, foxes, cats, dogs, cattle—even mongooses in Puerto Rico, but we’re not tracking the numbers of suicides in medical students and doctors. Do you ever get the feeling you might be less important than a Puerto Rican mongoose?
Here’s what scares Kaitlyn’s dad. Now I want to preface this with something else I learned about Kaitlyn’s mom who also suffered from depression. I asked Kaitlyn’s dad when his wife developed depression. Get ready for this. He told me it was after she completed nursing school in her 30s when she worked in a nursing home with a high census in which she was witnessing unsafe conditions for patients—and staff. She was normal before nursing school. Okay. Normal. Like medical students who start med school with their mental health on par with their peers. Then something happens during medical training to doctors—and nurses.
This is what really scares Kaitlyn’s dad. He tells me, “I got one child left. She’s in nursing school. I hope she’ll beat the odds. I can’t handle another.” This man has a real risk of losing more people in his family than we lose in a year to rabies! What are we doing? For him? For medical students? For us? Here’s what we should be doing:
First: prevent healthy medical students and doctors from getting conditions that lead to suicide. Second: Early diagnosis, referral and therapy. Third: help suicidal medical students and doctors rehab.
Let’s start with a holistic and humane medical education that de-stigmatizes mental illness.
The goal: help medical students be the self-actualized doctors described in their personal statements for which they were accepted into medical school in the first place. We know how to grow happy and healthy people. This is not some sort of secret. Follow Maslow’s Hierarchy of Needs. Begin by meeting physiologic needs with adequate sleep, time to eat and bathroom breaks. Simple. Basic. Ya know? Meet safety needs with a safe workplace without bullying or abuse. Social needs can be met by allowing students to feel part of a community with time for intimate friendships. And finally, self esteem needs. Medical students should feel honored and respected for their contributions and level of mastery in medicine. Not belittled. Not shamed. Not pimped. Not hazed. This is 2014.
Meet social needs with Matched Mentorship Programs. Use match.com technology to match first year medical students with second years—and physicians within their specialty of interest. Match Day should be the first week of medical school. Don’t wait until fourth year for Match Day. These people need friends. Now. We should not allow medical students like Kaitlyn to die from extreme loneliness. Meet safety and self-esteem needs using nonviolent communication (NVC) which is based on the premise that every behavior is an attempt to meet a need. We can try to change others’ behaviors by using shame and blame or we can listen and educate compassionately. If you hear a doctor raise his voice at Vincent, would you pass by unsure of what to say? Meet the conflict with confidence using NVC using a simple 4-sentence sequence—a stated observation, feeling, need, and request.
Observation: I heard you speaking loudly to Vincent. Feeling: I feel concerned, because . . . Need: I need everyone be respected in this hospital. Request: Would you be willing to lower your volume and speak with more consideration for Vincent’s feelings?
Meet social and self-esteem needs with Balint groups. These are small group clinical case presentations that focus on the patient-physician relationship and enhance our ability to care for patients. Balint groups are usually led by a doctor with some experience in facilitating these groups and/or a psychologist/counselor. These groups are easy to start. If you want some training, I’d recommend the American Balint Society. Has anyone here ever done a Balint group? (Lots of family docs raise their hands in the room).
If Vincent could have attended a Balint group, he might have shared, “This week I saw a 30-year-old male who presented with injuries after jumping from a 3-story window after raping a young girl. I was tachycardic and I had trouble maintaining eye contact . . .” Vincent would have the chance to share feelings and get feedback in a safe environment. Offer Balint groups at lunchtime and meet physiologic needs too since students do need to eat! Ya know, give them a Subway sandwich or something to share.
Early intervention begins with a yearly physical. In Kaitlyn’s second-year physical her doctor might have said, “I see you lost 20 pounds since first year and you’re getting up at 5:00 am to run 10 miles before class. How are things going for you?”
Every medical school needs a 24/7 helpline staffed by medical students. We learn to do blood pressures, ear and throat exams on each other, let’s learn emotional support too and give first and second years the real-world experience of being on call—for each other. Build in support for transitions from second to third year, traumatic cases, and medical errors. We’re all going to make an error and we should not have to feel like a failed perfectionist who can never be a good doctor. Again, medical students and physicians should not be left to cry themselves to sleep in their pillows alone at night with no support. That’s inhumane.
We need physician-specific rehab for substance use, physical, and mental health issues that are unique to physicians and medical students. Even medical students and residents with physical ailments feel ostracized from the group. The message usually goes something like this: “Let us know when you’re off the ventilator so we can put you back on the call schedule.” What kind of support is that? Rehab should be flexible, in town, with part-time work options. You know what kept Greg from drinking? His work. He loved working. Why send this excellent doctor 300 miles away? Greg shouldn’t leave town for inpatient rehab if local, output rehab is effective. And rehab should be non-shaming. When Greg called his mom (a psychiatrist) for help, his PHP therapist said, “Oh, you had to call your mommy?” What kind of treatment is that? We need personal physician oversight so our vulnerable colleagues are not abused and traumatized when they need help.
Would they be alive today? YES. Their deaths were 100% preventable. Every day we don’t take action, we lose another Kaitlyn, Vincent, or Greg. So what will you do?
1) Will you talk about physician suicide? If you lose a peer, will you hold an M&M conference or perform a psychological autopsy? A group of cyberspace docs recently asked me, “What gives you the right to perform a psychological autopsy? To go through these victims’ autopsies and suicide notes?” Well, these families reached out to me. I didn’t go looking for this. I didn’t even know I was doing psychological autopsies until I discovered the term in a suicide article. FYI: families with suicided children are eager for someone to take a sincere interest in their kids’ deaths. Would you be willing to honor their children? And prevent future deaths among your peers? Another gang of cyberspace docs wanted to know what kind of training I have that allows me to do these psychological autopsies. Do I have some sort of certificate that gives me the right to do this? I have no training. But my mom’s a psychiatrist. My dad’s a pathologist. Maybe that means I’m a natural at psychological autopsies. What training do you really need? Just take an interest in your dead colleagues. The only question you really need to ask is “WHY?”
2) Will you stop the bullying and abuse? We can all reach out to faculty who use shame-and-blame teaching, call attention to the violence, and offer alternatives. We do not need fear-based teaching to learn how to be healers.
3) Will you learn nonviolent communication? Vincent was inserted into violent crime scenes. Why speak violently to one another? NVC can reduce the trauma of our traumatic jobs. Let’s learn and then teach NVC. It’s easy. I learned in an hour online. Plus my ex-husband’s last girlfriend teaches it and I hired her for a private lesson. Takes about an hour—or at max two. Every medical school, hospital, and clinic should teach their students, physicians, staff—even administrators and CEOs how to speak with kindness and compassion.
4) Will you start a Balint group? All medical students and physicians would benefit from a weekly lunchtime case conference, a structured release valve for the trauma they have witnessed. Vincent and his peers could have processed their feelings and eaten. I teach a biannual physician retreat in which physicians often (spontaneously and without prompting) start crying about cases from years ago. One doc in her late 50s broke down about a miscarriage she witnessed over 20 years ago. She was just so happy that she could finally cry about it! She hadn’t been able to cry in years. Really? We’re just supposed to just shove all this down day after day, week after week, year after year with no release valve? You can’t tell your spouse. Cases are confidential. Plus you’ll wear out your spouse. There’s a reason most people don’t go into medicine. They can’t handle this stuff. We can IF we have a way to process our feelings in real time before we start plotting our suicides. Please (I’m begging you) start a Balint group in your clinic or hospital. You could save lives.
5) Will you reach out to troubled colleagues? Doctors like Greg won’t just come up to you and say, “I’m suicidal.” But he might say, “I had a rough day.” (That’s doctorspeak for I NEED HELP!) When docs e-mail me their troubles, I call them back immediately. Sometimes 30 seconds after they hit the “send” button on their computers. They’re shocked. I respond,” When you’re on call, you call patients immediately. Right? Why don’t we do that for each other?”
6) Will you be a mentor? At the time of Kaitlyn’s death she was dating a man in Michigan who was a 99% match on OkCupid. Kaitlyn needed a matched mentor in her own town—at her own school. Someone to watch over her. Could that have been you?
There’s so much we can do. I don’t care what you do as long as we do something. So will you go out on a limb to save a doctor? To save the people who dedicate their lives to saving others? And if you are suffering, will you seek help? Standing at the town meeting, I went out on limb. I didn’t just tell folks I was an unhappy doctor. I told my entire town I was depressed and suicidal. I begged strangers to help me design an ideal clinic. And define an ideal doctor. I had lost my way. They told me an ideal doctor has a big heart and a great love for people and service. And an ideal clinic is a sanctuary, a safe place, a place of wisdom where we can learn to live harmlessly, listen with empathy and observe without judgement. It’s a place where a revolution starts where we rediscover our priorities with relaxed appointments, smiley-face balloons and fun flannel gowns—a lady at the town meeting even volunteered to make them for me. Then a bearded guy in the back of the room raised his hand and asked a question I’ll never forget, “Is it possible to find a doctor who’s happy?” I collected 100 pages of written testimony, adopted 90% feedback and we opened one month later. That was 10 years ago. I’m happy now. All because I asked for help.
Pamela Wible, M.D., pioneered the first ideal clinic designed entirely by patients—the original “Patient Centered Medical Home.” She was once a suicidal doctor and now dedicates her life to helping medical students and doctors who are disgusted with, depressed by, and feeling suicidal about their once-beloved careers in medicine. There is hope! Come to the next physician retreat (premeds & med students welcomed). Learn more about the ideal medical care movement in Dr. Wible’s TEDx talk.
I believe we choose our parents before we are born. I hit the jackpot.
I picked an unlikely pair—a radical feminist and a guy named Ted Krouse. Mom wasn’t home much (she was finishing up her psychiatry residency) so I became head of the household. Dad always kowtowed to the strongest woman in the room. I was two at the time. I never had a bed time or a bath time and I sent Dad out on midnight runs to 7-11 to get us Slurpees and chocolate bars for dinner. Since I rarely bathed, I ended up with dreadlocks. Dad turned my poor hygiene into a neighborhood contest. The kids on the block lined up in our living room. Dad gave $1 to anyone who could move a comb through my hair.
Ted was basically a single dad. Every so often he’d place an ad in the newspaper for a live-in nanny. A slew of women from all over town showed up at our doorstep to compete for the position. Dad lined them up across the piano bench and onto the couch. Then he’d point to me and my baby brother on the floor and ask, “Do you think you can handle them?” None lasted long. Some quit mid-shift, I think a few on their first day.
With unreliable child care, I’d accompany Dad to work. The morgue was like our secret clubhouse. Dad would open the stainless-steel doors to the cooler and say, “Good morning! Is anyone home?” He’d prop me up and introduce me to all his patients.
Then we’d head to the Camden methadone clinic. As clients came in, Dad introduced me “This is Pamela. She’s a doctor-in-training. Show her your track marks.” Then he’d tell them a secret: “Ya know, I got an addiction too.” Opening his drawer, he pulls out a bag of banana-flavored marshmallow candies. “I love Circus Peanuts, but I’ve had this unopened bag in my desk for two years. I don’t allow my addiction to control me.” I’ve never seen anyone eat these—except Dad. His secret to longevity: cigarettes, vodka, and Circus Peanuts. At noon, he gave lunch money to clients in need. He hands ten bucks to a trans woman and tells us to “go have fun.” So I spend the afternoon on a street corner with recovering heroin users, eating pizza, and learning Spanish slang from a sexy Puerto Rican woman with huge biceps.
At nightfall, we head to the jail, where we evaluate drunk drivers. While most kids are preparing milk and cookies for Santa, Dad and I spend Christmas Eve seeing 30 prisoners on night shift. We set up our cots in our own cinder-block room with Dr. Krouse displayed prominently on the door. I watch drunk black men staggering in and out of our bedroom all night long. Dad introduces me as a “doctor-in-training,” then tells the men, “Lean forward and breathe toward me.” He sniffs them for alcohol. Dad was the City of Philadelphia’s human breathalyzer. Ted’s nose saved lives and kept Philadelphia streets safe for over 20 years. My father had nearly 14,000 guys with DUIs breath and burp in his face—until they replaced him with a mechanical breathalyzer in the 80s.
We spent nights at the state psychiatric hospital hanging out with schizophrenics plus we were on call for the Fire Department. We’d end up at midnight apartment fires in crime-ridden neighborhoods. To keep us safe, Dad bundled us up and locked us in the car. I’d wake my brother, unlock the door, and drag his little body over firehoses until we were stopped at the police line. The magic words, “I’m Dr. Krouse’s daughter” and they’d let us wander off right toward the fire.
Dad, you shielded me from nothing. You exposed me to sexuality, racism, poverty and death—all before starting grade school. Thank you for your courage. You weaned me from the bottle and let me to drink from the cup of truth. You never censored me. And you never censored the world around me. I didn’t understand the value of your gifts until I was older.
On birthdays and holidays, when most girls get chocolates or flowers from their fathers, you sent me a Valentine’s Day box of Godiva gallstones (the most beautiful gemstones that you retrieved from real gallbladders just for me). You sent me gift boxes with heart valves, kidney stones, and prosthetic testicles—along with my birthday cards.
You called yourself my first boyfriend and told me our solid relationship would pave the way for a lifetime of loving relationships with men. Actually Dad, you made it kinda difficult for me to find a date. Strong, eccentric, fearless females who prefer spending Saturday nights in the morgue aren’t in high demand. While my Wellesley classmates were seeking husbands at Harvard and M.I.T. frat parties, I took the night shift at the homeless shelter where people mistook me for a light-skinned black woman.
You treated all people with honor and respect whether they were black, white, Puerto Rican, whether they were on heroin, alcohol, or homeless, or dead. Ever nonjudgmental, with a heart of compassion. Your benevolent service inspires me every day to serve people with an open heart. I still do house calls just like you and—like you I’ve never turned anyone away for lack of money.
I want you to know that the people you exposed me to were more than your patients to me. They became family. You made the entire world my family. And you made me a family physician to the world.
You took me to work and now I’m taking you with me. You are scattered in stories throughout my books, on national TV interviews, on websites, and blogs—and in all my talks to medical students and physicians. For 46 years I tagged along with you. Tag along with me for the next 46. Our adventures have just begun. Rest up. You’re coming with me next week when I present my work on physician suicide to 5,000 physicians in Washington, DC. Dad, I know you really, really wanted me to be surgeon general, but our professional influence has surpassed the confines of the office of surgeon general. I hope you understand. I don’t need medals or fancy titles. Medicine is an apprenticeship profession. And I learned from the best man out there.
YOU. The one-and-only Dr. Theodore Krouse—you are SO eccentric. Ya know, you’re the reason I’ve never owned a TV. Nothing on television can ever touch my real-life adventures with you.
So I want to thank you. For everything. For never hiding the truth in happily-ever-after children’s stories. For never sheltering me in a hollow make-believe world. For introducing me on day one as a doctor-in-training. As healers, you and I are fueled by tragedy and we are forever intertwined in our pursuit of tikkun olam—a more perfect world.
In the end, we are all just spiritual beings having a brief and finite human experience. Thank you for choosing to share your human experience with me. It’s been an absolute blast. But above all—more than anything else—I need to thank you for never taming my hair or my spirit.
Bless you. Be free. . . .
Pamela L. Wible, M.D., is the founder of the ideal medical care movement. To learn more about ideal medical care, watch her TED talk. Here she delivers a final TED talk for her father, Dr. Ted Krouse (9/18/23 – 10/10/14).
Pamela, get this—after saying that I’d need to make up for my ‘lost time’ on production since I’m quitting my job and taking off for our retreat, the Head Suit calls me today and begs me not to quit. I’m talking shamelessly groveling, tail-between-the-legs PLEADING in this phone call:
Suit: “Don’t leave. Please. I don’t want you to go.”
Me: “Um, okay.” Wasn’t sure what to say to that. Totally different attitude than when we were talking 3 days ago about my subpar “production.”
Awkward silence.
Suit: “Is there anything that would keep you here? Anything?”
Me: “Well, um, honestly?”
Suit: “Of course! I want you to be totally honest.”
Me: “Okay. Then no.” Pamela, this whole process is crazy-making. I feel like I’m in my abusive first marriage all over again! But at least I got nice flowers and makeup sex out of that!
After reading her above e-mail, I reply: “Can I publish this?
Her response: “Oh HELL YEAH!!!! I would be completely and utterly honored. But please include one final note:
Dear Suit: Word to the Wise: Don’t ever try to mind-fuck a psychiatrist. Sincerely, Dr. Out-The-Door”
Pamela Wible, M.D., is a family physician and founder of the ideal medical care movement. Watch her TEDx talk on ideal care. If you’re a doctor, join the physician teleseminar and learn how you can stop taking this shit and start practicing real medicine. Photo by GeVe.
I delivered this presentation on August, 28, 2014, to medical students at the College of Osteopathic Medicine of the Pacific-Northwest and received my first standing ovation. Transcript and videos below.
Introduction: Pamela Wible, M.D., is a family physician born into a family of physicians. Her parents warned her not to pursue medicine. She did it anyway, but found neither doctors nor patients were happy. So she led town hall meetings where she invited her community to design an ideal clinic. Wible’s pioneering model has been replicated nationwide. Her model is featured in Harvard School of Public Health’s Renegotiating Health Care, a textbook examining major trends with the potential to change the dynamics of health care. Dr. Wible is author of Pet Goats & Pap Smears, Amazon’s #1 top-rated medical e-book in 2013 (and Amazon’s #1 best seller Physician Suicide Letters—Answered). Her essay on physician suicide in last month’s Washington Post was the third most read national news story of the day. Dr. Wible has been interviewed by CNN, ABC, CBS, and she is a frequent guest on NPR. Today she shares how to graduate from medical school without loosing your soul in her presentation “First Do No Harm—To Yourself.” Please welcome Dr. Wible . . .
Warning: Bouncy video.
Dr. Wible: Thank you for having me! I just want to congratulate you all for getting to this stage in your life. Isn’t it awesome? You are finally in medical school, some of you. And some of you have survived a year or two. Is anyone a fourth year? Okay. They’re all on rotations. Third years? So it’s all first two years. Wow. That was the most brutal part for me. So anyway, everyone gets a Pet Goats & Pap Smears book. I wrote that specifically for medical students to show them that there is literally a light the end of the tunnel. Sometimes if you can’t see where you are going, life is very confusing and nothing makes sense.
So the secret to surviving medical school is to DREAM BIG. You need to have a big dream for your future. You already have one because you wrote it on your personal statement. And only you can keep your dream alive. I’m going to share what happened to three medical students who were not able to keep their dreams alive—and one medical student who did. Meet Kaitlyn Elkins:
I’m going to read a letter that Kaitlyn’s mother, Rhonda Elkins, wrote. (to read Kaitlyn’s suicide letter and the suicide letters of other medical students and physicians, please see Physician Suicide Letters—Answered)
On April 11, I got the most dreaded call that any parent could ever get—a call from the police in the town where my 23-year-old daughter, Kaitlyn, was starting her third year of medical school at Wake Forest. He said he had to talk with me about my daughter. . . The blood left my body as he told me what happened. He said that she was deceased. . . He said that she had taken her own life. My world and everything I’ve ever known came crashing to an end at that moment.
How could this have happened? My daughter seemed to be the most together person I have ever known in my life. Graduated valedictorian from Whiteville High School, summa cum laude from Campbell University in two-and-a-half years and accepted to medical school, where she could pursue her lifelong dream of being a doctor. And she was doing extremely well in it.
She had just taken a Step One medical board exam and felt she had done well. An artist, a writer, an avid runner, she had common sense and was wise well beyond her years. She was excelling and seemed to have the world in her grasp.
I had just seen Kaitlyn the weekend before at Easter. We had a wonderful mother-daughter day, went shopping, out to eat and the movies. She seemed totally happy. How could this have happened?
How COULD this have happened?
This week we lost two more. In New York City. Both newly graduated from med school. Sean O’Rourke was 26 when he jumped from the 26 floor and died on 26th street. (weirdly, his mom’s name is Rhonda and sister is Kaitlyn). And the other one was only 25 years old when he jumped out of New York Presbyterian Hospital a few days later.
And I lost both men I dated in med school to suicide. Not during medical school, but later. And here they are. And so this is like a really big problem and that’s why I’m obsessed and I can’t get off this topic until we address it in a serious way because it does deserve serious attention. And I really wish I could interview these people who just died, but of course I can’t. I would just love to know what their chief complaint is. You know. Since they’re dead, I sort of feel compelled to do an autopsy on myself—a psychological autopsy on the mind of a medical student. So this is not that easy to do, but I did dig up my diary that I kept during medical school 25 or so years ago, my yearbook, my assignments here, I have letters. I had to read through all this. And I put it off for a long time because I didn’t want to read it because it was really painful to be there so I really didn’t want to dig through it, but since I want to know what’s happening with these people who are dying I just decided to dive in to some pretty heavy material and what I discovered was pretty horrifying some of the things I read, but there was some interesting surprises. You know 20-25 years into the future to look at this with the wisdom I have now.
(Note: during Kaitlyn & Rhonda’s portion of my talk, videocamera suddenly stalled. Warning: video is a little jumpy)
FIRST YEAROF MEDICAL SCHOOL:
So first of all I would say, like most medical students, I started first year really happy and excited. I was finally getting my dream off the ground. And, you know, I was excited about everything. I was excited about my apartment. I was excited about my new puppy. I was excited to hear mens’ voices—even with this Texas twang—because I was at this at uppity east coast all-women’s college for four years so I hadn’t really been around men for a while so the whole thing was new and interesting and exciting and I was, you know, even excited to get Bs and Cs in my classes on tests because I thought that’s still pretty good being in medical school. I wasn’t getting straight As anymore. I was fine with all of that.
TWO MONTHS INTO MY FIRST YEAR:
And then two months into my first year of medical school, I got extremely depressed which continued for the next two years and it was horrible. I was crying every night. I did tell my parents because I thought they could help me because they’re physicians so obviously they went through this before, but they were really useless. Honestly, there was nothing they could do to help me. My mom did send me some antidepressants and sleeping pills which didn’t help. And so I was just kind of alone in my apartment crying with my dog feeling miserable and I just felt like my soul was dying. It was the worst feeling ever. And it wasn’t because of academics. It was because of the culture of medicine—it just absolutely made me sick. And it was just really strange because I was so alone and I had to figure out what to do all by myself. Nobody else in my class seemed to be so depressed.
Between episodes of crying, I did start to develop this extreme perfectionism about my personal life which was new for me. Like even though nobody in my town was recycling that I knew of, I started recycling everything. I had everything completely organized even though I had nowhere to take it and I didn’t own a car. I was recycling everything. I didn’t want anything to go in the trash. I became a strict vegan. I was taking in stray animals. Today it dawned on me why I did this. I think it’s because I saw so much unethical behavior in my medical school that was so hypocritical that I just on the other end went extremely ethical, perfectionist. Like to somehow counteract what I was seeing which I thought was undermining the human spirit and I did not want my soul to die so I was on top of it every day doing everything I could and then I even wrote in my diary: “I will not consent directly or indirectly to participation in any abusive system. In order to achieve my vision I must be strong. I must adhere to what is GOOD—walk away from what is WRONG.” I just had to constantly (between crying episodes) like keep reminding myself of what I was trying to do in my life because I felt like everything was trying to crush me.
So then what really threw me off and I had no idea it was coming is these dog labs that we had to do in my school so that I was reading in the instructions what was coming next: Four students assigned to each dog in “Events of the cardiac cycle” lab where we had to inject into a live dog epinephrine and then study the EKG. The dog was probably already stressed out, but whatever. Study the EKG which probably doesn’t look too good and then cut the cardiac nerves, slice open their chest, shock their hearts—like give them a heart attack. Really? A dog? And then cut their hearts out and take our scissor blade and stick it in the aorta and slice it down into the ventricle and check to see if they have heartworms and then throw their body—dispose of their carcass and then clean your instruments and your work station.
There was just no way. I was ethical vegan. There was just no way I was going to sit and kill a dog to try to become a doctor. It just didn’t make any sense at all. Oh, I kind of just lost it. So I went and signed the papers to drop out of medical school because I just couldn’t take it. It was just way over the top.
Then I realized after I signed the papers that I didn’t have any money to get a U-Haul because I spent it all on my tuition and my apartment so it’s not like I could go anywhere so then I had dropped out of medical school, but I was stuck at my medical school at the same time. Sitting on this bench outside the library when my anatomy partner walked by who’s really like a super common sense kind of guy and I explained my predicament and he said, “Well, why don’t you keep taking tests and see what happens?” (I obviously took his advice and then graduated)
But I still had to figure out what to do about this dog lab because I wasn’t gonna do it. So it just dawned on me driving here that was the fight-of-flight moment of my life. I was trying to flight, but it did not work. So then I went into complete fight mode. I’m usually a very agreeable nice person, but at this moment I wrote a letter to the chairman of the physiology department and said just an FYI—I’m not going to be doing these animal experiments. Well, he wrote me right back and said, “these experiences are not experimental. Attendance is mandatory and there is no alternative to these experiences.” I mean, what could they give me that is an alternative to that? It’s pretty barbaric. He continues, “You have been placed on team 11B” and he told me when I have to show up and “failure to participate in this experience will compromise the learning experience for your fellow teammates and will be an unexcused absence and result in your getting an incomplete grade which is required in order to matriculate into the clinical core.” So he pretty much said I was screwed.
Interesting: I didn’t read you the whole letter, but there was a part here that said, “If you had objections to participation in this laboratory you should have petitioned the Dean of Medicine.” I think this is what I totally got re-reading this 25 years later. I really got hung up on that word petition because I literally got out a petition and started circulating it around my class. It said: We the undersigned feel that labs involving the use of live animals are unnecessary or unjustified due to our moral beliefs. We, therefore, ask that we be exempted from or offered an alternative to these labs in our medical school education.
There were 189 students in my class and a total of 4 people signed it. So that’s the situation Only 4 people thought it was wrong to do that and (quick math) 185 people thought that was okay! That kind of pissed me off. But I was glad I got 4 people, me being one of them so I got 3 other people besides me who thought there was something wrong with this. But I was still in this massive adrenaline fight mode which is kind of interesting for a 22 year old to go against her entire medical school and all these guys who are in their 50s and 60s in mahogany offices who don’t have to do anything you say. They could just kick you out and replace you with somebody else so it’s not like I’m in the driver’s seat or anything. But I sort of acted like I was—and it was effective.
I created another petition which was essentially “I support my classmates right to choose based on their religious and philosophical beliefs not to participate in these labs” and I circulated that around and I got ZERO people to sign! That sucks! I threw that one away. I can’t even find it. I just didn’t save my blank petition. But I did mail this one (with the 4 signatures) to the Dean of Medicine, George Bryan, who made me meet with him and he diagnosed me in his big office there. . . I was just so mad it was hard for me to have any kind of empathy for anyone that was trying to do this to me, but reading this stuff later it is kind of interesting because I think he was a nice guy, but I was just so worked up. I think he thought I was interesting too, but he diagnosed me with BAMBI SYNDROME and he basically exempted me from doing all these live animal experiments which there were more than just the dogs. There was the hypovolemia experiments on the sheep and all the other stuff we had to do where they re-use animals every year that are completely freaked out being around humans. It’s just unbelievable.
So I didn’t have to do it. That’s awesome, but then I really went out on a limb. I still must have been in fight mode because I wrote this amazing anti-vivisection piece that I submitted to the city paper and they printed it in the op-ed section which is super bold for a first-year medical student to just go out into the public and say all this stuff is wrong and have it printed in the newspaper. So I’m giving you copies of all this when you leave because I like to encourage everyone to stand up for themselves. Like the sooner we do it, the better our profession is gonna be.
Then every year (and I do recommend this for medical students)—every year I kinda wrote a little summary of how I did in medical school and I did a mass mailing to all my friends which is pretty easy now with the Internet, but I actually typewrote stuff with a typewriter and put them in envelopes and everything just so people could keep informed with my life so here’s an excerpt from what I wrote about my first year in medical school:
Incomprehensible to me, it seems the majority of people condone the use of live dogs for first-year medical students to carve on with absolutely no surgical skills and little idea of what they are doing and how it fits into the greater scheme of things. With the hearts cut out, blood on their hands, and fifty carcasses in tidy plastic bags, another class of medical students is on its way to becoming “healers” of our society. Why are the screams of the helpless and powerless animals unheard by the students? What implication does this have for the helpless and powerless in society seeking health care? And why is life taken so lightly? These are basic questions I continue to ponder. If nothing more this year has taught me about human nature, the difficult fight against power structures and institutionalized systems, and most importantly how to be consistent and strong in my beliefs. (which I highly recommend for everyone even though it is hard and scary)
So then I still had to be in the building while everyone in my class did these dog labs and I didn’t even quite get that until I was in histology and all these dogs with their wagging tails went by the door and then I was literally panicking with tunnel vision, tachycardia. I went into a full blown panic attack because in the next room, right on the other side of the wall where I am studying histology, my classmates are being (in my opinion) like methodically dehumanized right in front of me and it was just super out-of-body-experience painful. And of course my classmates came out covered in blood. And yes, they removed the dogs’ hearts—and they also removed their own hearts. It’s just really weird because these are all my classmates who are somewhat heartless now having had that experience (which there was no alternative to).
So then I started noticing that people in first and second year were starting to crack. Like a guy got arrested for masturbating in the parking lots of a grocery store. A woman in my class raided her parents bank account and ran off to Mexico. Two people killed themselves the year ahead of me in a drunk driving accident off the seawall into the ocean. A guy in my class got in trouble with the police for pedophilia. Like everywhere I turned after that I saw people crack completely open and just lose it. Because it is not normal what they ask us to do. We all have a cracking point. Mine must be somewhat higher. This is not the way to train doctors.
I’m always hopeful that it is better now. I think it is. They still kill pigs at OHSU for first-year medical students. I don’t know what they do here. Hopefully none of that.
Oh the other thing about my school. We have fraternities at my medical school. I went to an all-women’s college. I wasn’t really around men. I don’t know. Everyone is running around drinking naked jumping through fire hoops. They’re driving around in a car that says, “Trust me. I’m a doctor.” Oh my gosh! It was a combination of the worst juvenile behavior and scary this stuff. I just couldn’t believe it was happening.
THIRD YEAR OF MEDICAL SCHOOL:
The good new is then I started third year and it was AWESOME!!! Third year is great because you are finally with patients which is why you did all of this. Right? So I just loved third year. Every time I was with a patient my personal pain just melted away because I just got lost in their pain which was so much better than focusing on all my problems. And I realized reading through my diaries, all the trauma that I experienced came at the hands of my classmates and my instructors. I did not experience any trauma with patients—those were the good times—watching people die and inserting chest tubes. That was great! It was all the rest of the time when I am around these people who have been dehumanized and aren’t responding normally like with the normal amount of empathy they had before medical school and it’s just not a really good environment. So I’m going to read you two things that I found in the third-year portion of my diary.
Diary Entry – October 21, 1991: In the morning I found my cat killed by a car. When I arrived late for pediatric hematology, I was unsure whether my excuse would be well taken. Dr. Oblender said I could take 5 minutes to pull myself together which was unexpected considering I’ve had to listen to her make comments in the recent past about a cat not being any flatter after being run over more than once when a point is redundant. We all went to see a patient with ALL (Acute Lymphocytic Leukemia) and she proceeded to tell a story about a cat which I though was a little strange and insensitive. In conference that afternoon, a doctor came in saying, “Wanna see the control?” and a soft white baby bunny was in her hand with a #3 written on its back. I hesitated to touch her. I had her in my hands. I hope she could feel my love while the doctor spoke nonchalantly about whether maternal deprivation should be part of the experiment. . . .and it’s a hell that never ends. . .
And this is just what I had to deal with everyday. If we haven’t figured out by 1991 that maternal deprivation isn’t a good idea and that depriving medical students of emotions isn’t a good idea. Like we have to take little baby bunnies . . . Ugh. . . I could just go on and on . . . and then I found the page in my diary for which I was avoiding reading my diary for 25 years. This is the one thing that I did NOT want to read again and I found it and so I wasn’t originally going to read it to you, but I think I’m just going to go out on a limb and read it out loud. These are notes that I took during a surgery grand rounds.
Surgery Grand Rounds Notes: Good morning Pamela. Pull X-ray on Mr. Johnson. Take sutures out of Ortiz “ . . . and our animals are retuned to their metabolic cages. . . the animal awakens, shivers, and spreads the agent . . . and is sacrificed anywhere from 7 – 21 days.” It’s May 6, 1992. Surgery Grand Rounds and I can’t turn off the voices. I’m required to be here. But I will not view the slides. Stare at the wall, the floor—anything. Melt away. Fly away. Another attempt to escape the pain I have known for 3 years (I was literally in the back of the room crying trying to figure out how to make it through this grand rounds). It’s so deep.
(Shriner’s Burn Center was right next to us where they burn animals without anesthesia and they do it all the time and in my apartment I had to think about all the animals and all the things that were going on that were just horrendous crimes against sentient beings everywhere around me. It was like super hard to sleep that’s why I don’t know if I mentioned earlier I cried so much that my eyelids were sealed shut in the morning and sometimes I couldn’t go to class because I couldn’t even open my eyes and I had to feel my way to the bathroom is how horrible this was for me. And you might not share my views on vivisection, but I’m sure you have ethical and moral stances on issues and according to studies most medical students are put into situations where they’re having to participate in things that are unethical for them, but they somehow succumb to doing it to get their degree. But it only gets worse if you don’t stand up for yourself. anyway . . . continuing with my surgery grand round notes below:)
Another attempt to escape the pain I have know for 3 years. It’s so deep. The images imprinted on my soul. Flashbacks. The dog labs. Sure, I still see their tails wagging. The sheep blurred in my vision from my tears. “Once we characterize the wound healing in small animals we can move to large animals.” In the middle of an auditorium so large and gaudy like a five-star hotel surrounded by death. Where does the money come from? I said to Glen. Makes me feel as if there are no social problems beyond these buildings. Bordering on ludicrous. He assured me it’s for a good cause. Humane research. Only when it’s necessary. FUCK YOU! There’s the “Diabetic mouse. . .” Don’t look at the screen. Out of my left eye I see the pretty white fur—blood soaked. One of God’s own. Pamela, feel it. Know their pain. Protect yourself. Be strong. You can’t cry here. They don’t understand you. “ . . . added endotoxin to the model . . .” Nude rat—athymic, a splenic a genetic clone, patented. These mother fuckers. I hate them. Wait, I can’t do that. I have to love my fellow man. The sheep model is good because we can get large skin flaps. You can look at nerve division. I have to love them. How? Oh, have a nice day. Take a deep breath, Pamela. Ok. Fine. I’m in a room of cadavers—physiologically living, spiritually and emotionally dead. Trapped in some sort of wealthy medical complex in Texas.
So these were the kind of notes I was taking in class. It was very out-of-body weird. Okay. And I had to get a lot of therapy after medical school to heal from this. I’m hoping you guys don’t have to experience the trauma that I did, then I entered fourth year!!
FOURTH YEAR OF MEDICAL SCHOOL:
Fourth year was AWESOME again!! Fourth year is like the home stretch. You can see that you can’t be stopped. It was really wonderful and a really cool thing happened the month before I graduated I realized that I had a secret admirer in administration. And I didn’t really know this until sitting in Denny’s two night ago at 4:00 am when I had the willpower to sit and read through all this. But what happened is that in my third and fourth year because I love patients I was writing their stories. Kind of like a precursor to Pet Goats & Pap Smears. I just thought people had such cool life stories and I wanted to remember them so I started journaling those which was much better than writing about the things I just read you. So some of them actually got published in the student magazine at our school and so like this house call that I did to the Mathis family. They published it. And then I got wind of this memorandum that came by and it was written by my secret admirer’s secretary. Guess who my secret admirer was? The Dean of the medical school who let me out of the animal labs which I did not figure this out until yesterday! I’m reading the memorandum and it says:
Attached please find a copy of an article from a recent edition of “Omni,” the publication of the Student Government Association. Doctor Bryan has suggested that your office might be interested in interviewing the medical student who wrote this piece since it shows how our students do more than just go to school. He would really like to have the highlighted in some manner, particularly since she will soon graduate.
So they did this huge spread on me in the paper right around the time I graduated which was like awesome. It’s called “Medical students do more than simply attend classes.”
So in my medical school situation there were a lot of ups and downs. I wanted to share with you my trajectory because I think somehow since I can’t interview the people who are not here. I somehow think other people have the same trajectory—being really happy and then maybe getting depressed and then bouncing back. I do know that when students are with patients they have said their own problems melt away and that’s the only time they feel joy so I’m just sharing this with you because I think it is possibly what you can expect (except hopefully better). This was 25 years ago and I’m hopeful that things have changed, but very weirdly yesterday I got an e-mail from a friend of mine who said isn’t this your medical school? It was a Physician’s Committee For Responsible Medicine e-mail about how they are still trying to get them to remove live animals now from ATLS (Advanced Trauma Life Support) at my school. My medical school is now using goats for ATLS so I then got the opportunity yesterday to write a letter to remind them that I graduated like 20 years ago and was exempt from live animal labs and you guys are still using live animals so I’m just writing to respectfully ask you to consider using computer simulation or other sorts of things because I think we’ve come a long ay in 20 years and I’m a really good doctor and I didn’t go through these experiences that were mandatory and all that. So the great summary here is I have a top ten tips for loving medical school. I want you guys to know right now what you can do now to avoid some of these pitfalls. And I have handouts to give you that include all of my letters that I quoted because I think it is important for you to see that it IS possible for you to stand up for yourself and not be afraid and I think you will have people who will be secretly rooting for you and overtly rooting for you if you stand up for what you believe in. Think of what our profession could be if everyone did that. It would just be AWESOME!!! Like we wouldn’t need all this legislation to protect us from our patients and all these adversarial relationships that have developed and all these doctors jumping off of buildings. I just don’t think it would be happening.
MY TOP TEN TIPS FOR LOVING MEDICAL SCHOOL
1) LIVE YOUR DREAM FEARLESSLY ~ Be the doctor that you always imaged—like right NOW. Like don’t even wait to get your degree. Be that person now. Plaster your personal statement everywhere. Like all over your house, in your car, on your computer, put it in public bathrooms. Let everyone know what your plans are including sharing it with your colleagues because they can keep you accountable to your plans. You don’t just want to send in your personal statement and then never think about it again and then you graduate. You want everyone to know what your cool plans are which should be really big and awesome.
2) CRY FREELY ~ Show your emotions. When you stop crying you die. So crying more is better. That’s what saved me. I had to keep rinsing this stuff off that I was seeing every day.
3) REACH OUT ~ Ask for help & provide help. Don’t let classmates isolate themselves and withdraw. Start a buddy system. Befriend a classmate you have never met. This is what Rhonda Elkins said she wishes somebody would have done with her daughter because her daughter was kind of like a loner. She wrote a whole book about her beautiful daughter who was a valedictorian (like Sean who jumped off the building this week in NY). These people are amazing who are killing themselves. But if somebody would have just gone to their apartments and checked on them and just been their friends they wouldn’t be all alone. We are deep thinkers and empaths and we are sensitive and it is hard to be put through some of this coursework that we have to do (and hopefully it is better for you than it was for me). But still just having at least one friend in your class. . . and it does protect you if you’re married (like some of you are married with kids) because you automatically can burden your spouse with your problems. But what you want to really do is look for that person in your class that you don’t know yet and hang out with them and ask them out for tea.
4) ZERO TOLERANCE ~ for abuse, bullying, hazing, being mean. Come on. Human evolution. Aren’t we beyond that yet? Stand up for your classmates. When your classmates are berated and made fun of or an instructor is acting in a way that is hurtful to somebody, stand up and say something! Go to the classmate and say, “That was wrong.” Write a letter to somebody. If everyone in here wrote a letter after your exam tomorrow about something that you don’t like that is going on in your medical school, you could change things for the students this year and for people behind you who would not have to experience the same mean professor. Maybe he could go to therapy and get healed or something or have an exorcism. Really. There has got to be a way to help these people, but you should not let them pass on this mean bullying stuff to the next generation. If you can stand up for your classmates who are being abused and for yourself when you are being abused, you are going to be much better at standing up for vulnerable patients who are poor and come into the ER who get treated like crap. Why? The empathy burnout happened at the dog lab. So we have got to stand up for each other and be for real. And not allow cruelty to be going on anywhere. You are a healer. You are here to heal. You have to start with yourself and not let them make you do things that are unethical and not be afraid to stand up and say, “That’s against my religion.” And don’t let them hurt your classmates. That way later on you will not end up hurting patients—or animals—or anyone else who is depending on you to be a good steward on this planet.
5) DISLIKE SOMETHING? ~ Change it. I would really like to ask you all to write at least one letter this term to someone that could change something somewhere who can improve your life and the lives of people who come after you. It could be to someone in your medical school. It could be to a family member. To whom will YOU write a letter? SPEAK UP. Don’t ask what your medical school will do for you. What will you do for your medical school. Really it is up to you to create the learning environment that you want.
6) WRITE YOUR HEART OUT ~ You do not even need to go to a therapist. Writing stories was so therapeutic for me. And all my patients who are in the book are so excited because somebody thought they were important enough to write a story about (even if you use a different name) so it’s an honor for people when you write a story about them and it reminds you of the patients that you loved and enjoyed treating during medical school years and then 20 years from now hopefully you can reread your medical school diary and have a better reaction than I did when I read mine. I also recommend writing letters to friends which is easier now with the Internet. You don’t have to get out your typewriter. In the letters BE VULNERABLE and really share that you cried this term or this particular patient made you sad. It’s okay. You need to be a real human and alive.
7) SEE PATIENTS ASAP ~ Hopefully you have a curriculum that in your first year allows you to see a patient. If you don’t then volunteer at a clinic because that’s the thing that gives you energy and joy. If you are not offered a real patient in your first year, maybe that is a letter you can write. Can we please be assigned a patent in our first year?
8) BE LOVING & KIND ~ YOU are each other’s family and support for the next 4 years. Give classmates cards and flowers just for fun. Practice random acts of senseless joy with each other. It’s just gonna make it so much better for everyone. Right? Honestly, I really have a commitment here that you all will prevent anyone’s parents from getting a phone call from the police during the next 4 years saying that something happened to their child that was your classmate that you didn’t know. And you wished you would have met before they jumped or before they overdosed. That’s the call to action that I really have. I don’t want parents to be getting these phone calls anymore about people who are super smart and loving and all they ever wanted to do is help people. How can we let them end up in this situation?
9) FIND MENTORS ~ You need someone to believe in you and your dreams. It’s always helpful even if you just have one person who says, “YOU CAN DO IT!!!” Because there is so much cynicism in medicine you must have at least one person who believes in you. Why is there so much cynicism now? These doctors went through the same training I did. Your superiors had to do things that were unethical and they are still suffering from it.
10) EXPECT SECRET ADMIRERS ~ Do what’s right and you’ll have secret admirers. You might not figure out who they are for 25 years. But literally, oh my gosh, look I have this article in The Washington Post. Who started my writing career? The guy who I was scared of who let me out of the animal labs who encouraged the newspaper at my school to publish an article about me and he even said “her writing career.” I never even thought I had a writing career. They (Washington Post) offered me $50 for that article. I have a writing career now! I just think if you do what’s right you’ll have a lot of secret admirers and my big dream for all of you is not only will you have secret admirers. If you do what’s right you may even graduate with groupies & a fan club. 🙂 Better than a rock musician if you do what’s right. So that’s all I have to say. (Clapping)
This is my first standing ovation!! I think you are standing up for all these people too. These people who are helping us heal. Their lives were not in vain. Right? So I will take all the questions that you have and I’ll stay as long as it takes. Here’s another sweet guy who I love who was lost. I talk to these people’s parents. He died when he was 29. I went to Fed-Ex to photocopy these and laminate them and the woman behind the desk said, “Oh! Wow! Are they your kids?” And I said, “Yes. I think they are. I’m taking on their lives as seriously as their parents. Yes, They’re my kids. I’ve adopted them.”
So it’s about being a real healer. So please ask me questions.
QUESTIONS & ANSWERS:
Question: I was wondering if you could talk about the format on your clinic. How do you manage to put together a practice that really works for you and your patients.
Dr. Wible: Just to let you know I have a 14-page FAQ that is free if you e-mail me off my website that gives you all the nuts and bolts in 14 pages. How I set it up is that I basically just did what my patients wanted. They wanted small and simple and cozy. So I have a 280-square-foot office with one exam room. I can’t be in 3 exam rooms at once and I don’t want 3 naked people waiting for me at the same time. I just think that’s unhealthy no matter what your profession is. You should be focusing on one person at a time even if you are a hairdresser, even if you are a prostitute, even if you are a doctor, please just take on one person at a time. I think that’s how life works the best. So the thing is that cuts down the cost. My office space when I started renting it 10 years ago was only $280 per month and now it went up to $370 which is really cheap. I probably pay the least amount of almost any doctor on office space. And I have no staff so that’s zero on having to pay an employee. And my malpractice, by the way, is really cheap. Oregon is an awesome place to open ideal clinics because this is not a very litigious place like Miami or Chicago or other places where people seem to be sue-happy and juries tend to go against the doctor. Here it’s wholesome people who are just really nice who want a wholesome nice doctor so it’s a good place to live and reimbursement is really high in Oregon, by the way. Reimbursement is higher than anywhere else in the lower 48 that I’ve ever found. The only place that’s better is Alaska. The structure of my clinic is like any other clinic except I see one person at a time. It’s almost like a counseling office, but still do surgery, prescribe medication, take insurance. The only difference between me and a regular clinic is that I don’t give vaccines on site. Refrigeration is a hassle and they can get vaccines at any pharmacy now. For the most part I think you would feel like you were at any other clinic except you would feel like you were with somebody who is more maternal and loving and spends 30-60 minute with you. So you just don’t feel shuffled through.
Question: We learned in our behavioral medicine psychology course about the prevalence of suicide rates in physicians—especially older male physicians—and mental illness aside and everything with that seriousness what are the steps as physicians, male and female no matter what age we are, so that we don’t get bogged down by our profession and we don’t lose the vision while we are practicing. I definitely agree with something you said earlier—having a social support system, being married, having friends and family and colleagues. What are some other things we can do to safeguard ourselves and those among us?
Dr. Wible: One thing that I think you should be doing—including in your medical education and I hope somebody will write this letter and get this started is something called Balint groups. Have you ever heard of that? You can just look it up. There is even a Balint Society. Mostly doctors would get together. I experienced this at PeaceHealth Medical Group, which is one of my unfavorite factory jobs. But the doctors again don’t wait for their employer to do something for them. Do something for yourself. They put together these Balint groups in the family medicine department. So that was optional that you could come after work and sit 5 – 7 doctors and they run it like any other case conference sort of thing. Like one person will start and say something like, “I had a three-year-old patient who came in today with a Wilm’s tumor and I started to feel really sad because I lost my nephew to this. So what happens is you start by presenting a case but the purpose is not to discuss the differential diagnosis and to work on the patient. The purpose is to turn it around and talk about providing care for your patient with this condition because, you know, come on let’s just face it, you are going to see patients who are dying of things that your parents or grandparents have died from and you’re going to feel certain emotions around certain illnesses that are going to remind you of, you’re going to see patients that are going to remind you of family members and you are going to have a reaction to it and you can’t just—here’s the thing that’s not normal, it’s absolutely NOT normal to go in and work in the ER and tell a family that, “Sorry your 3-year-old died in the car accident” and they’re shrieking and screaming and then they tell you to just go in room 10 now and see Mrs. Jones because she is having a heart attack. And you go through your whole career sucking all that misery down without any release valve. You never go for help. You never talk about this. If you talk about any of this with your family members, you are going to overburden your family or people who are not in medicine. So I do think we need to heal each other because we can handle a lot of trauma or we wouldn’t be in this profession, and we need to help each other with these Balint groups, for example, a weekly group where you meet with first-year medical students or second-year medical students and you form a group of 5 – 7 people and you discuss like, Gee, learning about renal or nephrology or this particular disease is really hard for me because my mother had that and just be able to express how you are feeling so it’s not bottled up. WATCH an actual Balint Group here.
I lead these physician retreats(medical students welcomed!) and I had a woman come and actually start crying about a case she had 30 years ago. She said it was the first time she had cried in years and she was so glad she was even be crying and I’m thinking oh my gosh we’re just like piling this stuff on day after day, year after year, the traumas that we see especially because society isn’t quite functioning that well right now so we kinda serve as the social safety net for people and we’re hearing some really bad stories and then you just think you can take a nap and come back tomorrow and shove it all down again. So I think having Balint groups would be good which you can initiate at any time. And then also I think just being more human with your patients, like the whole professional closeness instead of professional distance.
I do think this is harder for men just because women are more relational by nature and the hugging and the estrogen and crying it just happens so easily, you know. I have a transexual patient on estrogen and to him (who’s now a her) I said, “How do you know you’re on the right dose? How are you feeling?” He’s like, “I’m so happy I can cry during movies now!” Okay. It’s good. Yeah. So the thing is you just want to see if you can stay connected.
When I see patients I try to connect with them physically (stethoscope on them, touch their hand and do something so that they feel like you touched them, right?) and then emotionally I try to connect with them and spiritually. Here’s something that can help ground the office visit. I always ask patients on the intake forms, “What is your life purpose?” and “What’s your vision for your life?” or something like that and then I write that at the top of their chart. Some people say just to “Live in the light of God” or to “Love my family.” But whatever they say it just really helps because then when you open the chart you’re looking at somebody and you’re seeing the whole purpose of the visit no matter what their physical ailment is he wants to experience God. This is his purpose for being on the planet. We’re just spiritual beings having a human experience.
And one thing I will say about men is that men generally even have trouble asking for directions when they’re lost in a car so to expect a guy with a white coat with all that ego and training to ask for mental health help is really asking a lot. Okay. So that’s why you need to build this in so that at the end you are not having an arterial bleed or jumping off buildings, ya know.
It’s about basically prevention by learning to have a release valve every week for your emotions, somehow, which is not burdensome to your family because you will totally wear out your spouse if you discuss the things you see at work. So a release valve with your colleagues. Does that help? Everyone look up Balint groups online and try to start those wherever you can. And by the way, since you guys are ahead of the curve here, I really do think that the younger generation of doctors is going to be healing the older generation of doctors who didn’t quite get as fair of a deal because we weren’t as evolved as humans back then because this was pretty barbaric what I had to witness. So anyway by you starting these Balint groups and talking about this when you are doing your rotations you can really help because you can really see that some of the people you do rotations with they don’t look that healthy and you don’t want them to jump, overdose, or grab a gun, so by starting these Balint groups at places where you work you would literally be saving other doctors’ lives, men and women. And you kind of normalize it because it is easier to say, “ I have a 33-year-old woman with abdominal pain” than go to a psychiatrist’s office and say, “I’m suicidal.” You know it’s much easier to start talking about the patient and then how you feel. And people don’t have so much faith in some of the wellness programs out there and they worry about the paper trail. There’s no paper trail with Balint groups. It’s just people hanging out together. Next?
(Wow, Transcribing this I see that I really drove home the Balint group thing. FYI: I have no financial interests to disclose regarding Balint groups 🙂 )
Question: Share some stories about how you have changed patients’ lives.
Dr. Wible: Well, just asking that question, “What is your life purpose?” on the intake form which is no effort on your part you just put an extra line after family history, allergies, and sneak in “What’s your life purpose?” and “What are your health goals?” Just by asking that you shift the whole relationship to “Wow. Nobody has asked me about my dreams.” And people will start thinking, “Why am I here?” It’s just amazing. I spent one entire visit with a curious 20-something guy who couldn’t get off what his life purpose was and we talked about that the entire visit. He left still wondering what his life purpose is and that was just more helpful that anything else I did during his physical. So one woman told me she felt like when she left my office that she had a physical, met with a marriage counselor, and had a spiritual awakening. So it’s like total one-stop shopping! So I think that’s what you want.
Basically if you’re practicing medicine well as a healer, you feel more invigorated at the end of the visit. If you feel more tired like somebody has drained you then you did not perform the visit correctly. Because in a real medical appointment both parties feel uplifted afterwards because you had like epiphanies, aha moments, connections, people figured things out about their lives at a deeper level. That’s what healing is. And when you actually have a healing experience even if you’re the one just witnessing it. it’s like a real rush of positive energy and so that’s how you’ll know if your appointments are going well.
Plus people leave with balloons and they’re smiling and one thing I did recently (you can check my blog and you guys should all be my Facebook friends!!! Look at my blog.) I had a patient come in and this is a friend of mine who every year she takes me out on my birthday with another friend of mine and they’re sometimes 6 months late taking me out for my birthday but they always remember eventually because I’m December 5th so I’m 12/5 and and my friend is 5/12 so we’re inverse birthday numbers so we always just kind of click and remember each others birthdays. Then our third friend who’s 8/23 doesn’t fit in our “numerologic clique” so I always forget to celebrate her birthday, but she’s always celebrating mine. Well she is my patient and she scheduled her physical on 8/22 and all year long I’ve been trying to remember 8/23, 8/23, I don’t want to forget Rachel’s birthday on the 23rd so what I did is I had a surprise birthday party for her in the exam room! I had all her friends back there with balloons and presents all over the exam table and when she came in it was super funny and he was there (my videographer and photographer) and so it’s all on there the video and everything. And when she came in it was so funny because she just thought she was with me, right? And I knew if she was going to talk about dry vaginas or anything I would have to cut her off because it’s like I didn’t want her to start talking about failed relationships or things that her kids wouldn’t want to listen to in the other room and stuff so when she came in it was so funny she said, “Hey sexy lady!” and we were hugging and we were laughing and you can tell we’re more than doctor and patient, we’re friends so then I said let’s go in the other room and do your physical around the corner and she was like, “Oh my God!” It was great! People were blowing horns and bubbles and so it’s just really fun to be playful about what you do because that’s healing. Check out the surprise birthday party physical!
Laughter is healing. In many offices the energy is low and the vibe is low and the colors aren’t so good and the doctors are kind of frowning. Guess what? Even when you are running in an assembly-line practice —> Remember this: you can accomplish just as much every day with a party hat on and it only costs 50 cents for a balloon. You can go to the dollar store and get helium balloons. Just having a balloon in the exam room with a smiley face. Anything. I even go to party supply stores and I look for stuff I can use on my patients. You know how when you are in exam rooms, especially in big clinics, they try to organize all the drawers the same: the KY jelly is here and here’s the hemoccult cards and so what I do is I always put my Mardi Gras supplies in there so everything is mixed up around the medical supplies so that I remember this is supposed to be FUN! So anyway . . . I mean you can literally code the same visit, bill the insurance company, do the same work smiling with a party atmosphere and actually you’ll both leave feeling better. I’m not kidding. It’s really easy.
Question: So we saw the clip of the doctor you helped open her clinic. Have their been any others locally recently?
Dr. Wible: She’s in Salem. Meet Lara Knudsen—the happy doc. And there’s like 10 in Eugene. Not all of them did town hall meetings, but they basically are running relationship-driven practices rather than production-driven. If you are in a production-driven clinic you feel one way. If you are in a relationship-driven clinic you feel another way. So what I am encouraging people to do (especially in primary care) is to have relationship-driven clinics because it just makes more sense. Doctors are happy and less likely to jump from a roof. It is protective to have relationships with your patients and to feel you are doing a humane amount of work. You should not ever feel like you are in an inhumane situation. If you are in an inhumane situation please write a letter about it to someone who can change that. Let them know that the situation is inhumane and use words like bullying, abuse, not in any kind of angry way. Some people may not even realize what they said borders on bullying and that the course load that you have and the hours you are keeping are like abuse. I think that’s new. We are bred to be self-neglectant. I heard a story of somebody in residency who’s marital partner committed suicide and she went right back to work the next day and didn’t take a breath. And that’s considered, “Wow! Great work doc!” That is not normal. We have to get to be human again and we need to remind people that inhumane situations are inhumane—for everyone, including the patient. It’s okay to be normal and human.
The reason why all of this is even happening is that there is a fatal flaw in reductionist medicine and we are still being taught the reductionist medical model. Reductionist medicine means that we’re machines so we’re like robots. You should be able to do your mother’s gallbladder surgery in a pinch. You know there’s an anesthesiologist who told me that in his program 10 – 20 years ago in Michigan, one of the students in his class had committed suicide and they took her body to the anatomy lab and made the first years dissect her. She was a third year. Whomever decided to do that to the students you’d think was super sadistic, but the people who are deciding these things they think that’s good for you! You should be able to in a pinch do the autopsy on your wife if you had to. Who else would do it? You should be able to! It’s ridiculous, right? Okay. Like we’re human. Hopefully our hearts are still in our bodies, our souls are still in our bodies. It will protect you from jumping off a building if you still have your heart and soul in your body and all your parts are working normally.
We can not put people in situations in which they have to turn off their humanity because eventually it gets permanently turned off. And they are not going to be good as parents. And they are not going to be good as wives or husbands. And they are not going to be any use to their patients. And they might want to die. And maybe that has something to do with our high rate of suicide. I would love to do debriefing interviews on these people. But I can’t. Maybe you can do a psychological autopsy on yourself sometime. It’s kind of fascinating. When you finish medical school just try to figure out what worked and what didn’t work. What feedback can I give so the next generation of doctors doesn’t have to undergo some of the stuff that didn’t work because it’s a group effort and we have to help each other and I don’t think anyone is really trying to harm us. We’re stuck. What do they say? A tradition is just a bad idea held by a lot of people for a really long time. Don’t we want to switch and do something more evolved at some point? So look at the mapand I have about 30 people in my teleseminar right now so just look up physician retreat on my webpage because I have scholarships for medical and premedical students. The 12-week course is $1600 for docs, but I have some students doing it for $300, some for free. If you want to do it that’s cool. We are only on week 3 and I have all the calls recorded so you’ll get to talk to me every Sunday at noon which I don’t know if you want to do that, but if you do here’s your chance!! And you can go to Breitenbush Hot springs with me in November like Claire did! Someone hand her a microphone. She has a testimonial.
Comment: (Claire, a second-year medical student) People who know me, I left school for a lot of reasons and I came back after a leave of absence. It definitely was life changing. A lot of people that went [to the retreat] they were kind of discouraged by the whole medical field in general. We’re really fortunate in the D.O. profession because a lot of people that come here are really well-rounded. So we kind of have a little bit of a different perspective. But from what I’ve seen even among doctors I really respect—I’ve seen how it’s taken a toll on their lives so it’s really refreshing to see how a bunch of individuals came together and how it changed their lives. Just finding the heart through medicine really. That’s what I really saw essentially. You can get lost in the paperwork, in the robotic atmosphere, but there is a very good way of putting your heart into it. It’s very, very doable and that’s why we’re here. Right? You have to keep reminding yourself why you are doing it and if you do that and always take care of yourself then you can really change lives.
Dr. Wible: Any other questions? I’ll stay as long as it takes. Here’s my physician suicide diary. Unfortunately, I’m still putting entries in every week. What else can I say that I have up here? You know it is really scary for people’s parents who have their kids in medical school now to see these articles, but like Rhonda said, if she just would have known that medical students have a high suicide rate. After accidents, suicide is the most likely cause of death for medical students. That’s why it is so important to have public awareness. It might take a while to change how we educate people and do some things differently, but at least if you even knew that your nephew or niece in medical school or your daughter was at higher risk, you would interact with them in a completely different way during medical school and so I think that’s why it is so important that we at least right now have public awareness. This is such a scary topic for patients. Nobody wants to hear about death and suicide is not something that anyone really wants to talk about and the thought that their doctors could be doing this. . . it’s almost like being Christian and finding out there’s no Jesus. It’s just too much. It’s too much for somebody to take that the way they’ve shaped their world. They hold doctors in a certain perspective and to find out that we are this injured is hard for even the media to wrap themselves around this which is why I’m amazed that I even got this one thing out there (referring to my Washington Post article). It’s baby steps, you know.
Question: So why are you an add-on at 6:00 at night rather than in part of the curriculum? I’m just curious about that. Have you been here before?
Dr. Wible: Yes. I did this before. He wants to know why I’m and add-on and why I’m not part of the main curriculum here. Well, I did this before in 2012. I think the reason, it’s a very interesting question because you know I don’t have a whole marketing team. I’m an M.D. and not a D.O. I have encouraged D.O.s in town who’ve opened ideal clinics to start teaching here. I didn’t even know if I would be invited. I’m not a D.O. I’m a lowly M.D. Really I would be open to teaching, but obviously my hands are full with a lot that I am doing. It’s something that if somebody asked me to start teaching at a medical school, I’d love to do it. I have not been asked to be a regular professor or teacher anywhere. It’s all generated by the interest of the students. Most events that I have done, its medical students who have invited me and the older doctors I just don’t have as much interaction with them. I have more interaction with the younger generation for some reason. Maybe I’m too youthful, I’m too playful. I think I might scare some people, you know. Honestly some of this stuff is hard to talk about with people who are older. I even have a woman in my teleseminar in fact I have several physicians who are suicidal in my teleseminar and interestingly when a relatively happy premed student speaks on the phone, later on when I’m talking to the doctor I discover they are actually angry at the younger person for being happy and I think it’s because they feel like they’ve lost their life dream and by hearing young people just on the verge of living their dreams, it kind of just digs it in for some people. So I don’t know that some doctors are even happy that I exist and that I am happy. I’ve had doctor be upset with me for being so happy. Literally on a listserve I was on some people thought I was lying about how much money I make and suspicious about how my office [overhead] can be so cheap.
I actually submitted an article to the American Family Physician. An article that I sent in (and I’ve been published in medical journals) it’s interesting because sometimes I run into these roadblocks. The journal was peer reviewed and they declined my article about community-designed ideal medical practices that embraced low-overhead because they said it was “too utopian in nature.” Okay. We want to stay miserable. I can’t force you to be too utopian if you’re not ready. So I don’t know. It’s too good to be true. They can’t believe I exist. I’m happy to be a part of your regular curriculum. Maybe that’s a letter you can write. Why aren’t we doing this?
Question: First of all thank you for coming. Your voice is a voice that’s needed to be heard for quite a while.
Dr. Wible: You need a microphone because I’m going to put this online because other medical schools would like to hear this too and they can’t believe I’m only doing this in Lebanon. How did you guys get so lucky?
Question: (again with mic) First of all thanks for coming. Your voice is a voice that’s needed to be heard for quite a while. I’ve been following you for about two years on . . .
Dr. Wible: Well, who are you? You’re stalking me.
Question: I’m Jay Anderson.
Dr. Wible: Jay’s been stalking me for 2 years.
Jay: So I left the software field because I felt that I actually needed more of a connection with people. And I can’t tell you the number of physicians that I spoke to before making my decision to leave the software field that discouraged me from pursuing this path and saying why would I leave and walk away from all that earning power. Well, because it’s soulless and empty. And they would tell me the direction I’m heading that’s how we feel. Why would you quit? Because I think there’s a difference that can be made. And I think that changing the ethic of the environment that we work in and what we’re working towards is how we do that. And I don’t think we can do that 10 minutes at a time so I’m very interested in the model that you’re proposing where we can sit and we can build relationships and that’s why I’ve been following you for the last couple of years. That’s why I’m stalking you. Thank you again.
Dr. Wible: You’re welcome. Yeah, I mean I think what people tend to do in the United States at least is we start demonizing different things like, “Oh it’s all the insurance companies fault” or “I don’t like Obamacare” or “It’s the pharmaceutical companies. They’re just rich and greedy.” There’s really nobody to demonize. Look in the mirror. How are you living your life? Are you a victim? You can NOT be a victim and a healer at the same time. The problem is our instructors in medical school too often feel like victims and this is an apprenticeship profession. If you are a victim as an instructor at a medical school you are creating a whole new generation of victims just by being there. I think we need to figure out who is not well in the teaching profession in medicine and get them the help they need so they can actually be what a doctor is which is a real teacher. You should not be teaching students if you are cynical and jaded.
Students that come to me in my office and at the end of the day when they shadow with me, I ask them, “Did this meet your goals?” or “Did you get anything out of this?” and they’ll say things like, “You’re the first happy doctor we’ve ever met.” Which is a great honor for me, but it really sucks thinking “Oh no! Wait, you’re in a medical school. You’re surrounded by doctors all day long and you haven’t met a happy doctor until you came to my office?” This is absolutely tragic! And no amount of legislation from Washington D.C. is going to reverse this okay if I’m the only happy doctor they’ve met. And they’ll say things like, “You’re the first solo doctor we’ve ever met. We were told in medical school that’s not possible anymore.” My question: “Who’s teaching medical school? Do they get out? There’s solo doctors all over the place and some of us are really happy. Other ones have recreated the rat race on a smaller scale and they’re not happy. We don’t have enough mentors.
Ya see, it should be like this (you all are getting a copy of this at the end, this handout here). On the reverse side of “Top Ten Tips for Loving Medical School” is the “The Healer’s Hierarchy of Needs.” I adapted “Maslow’s Hierarchy of Needs” to fit what doctors need. Okay we’ve got on the bottom PHYSIOLOGIC: * adequate sleep * bathroom breaks * wholesome meals & snacks * time to exercise * access to clean air & water * comfortable, warm clothing * sexually-fulfilling relationship * (I just made this up but you can add more, right?) then there’s SAFETY: *fulfilling work with freedom from malpractice fears * freedom from abusive third parties and Medicare/Medicaid pay cuts* freedom from threats of fraud investigation and dishonest employers * a safe workplace * nurturing environment * affordable health care and then there’s SOCIAL: *feeling like you’re an integral part of a community * giving/receiving love & affection joy of serving others * time for friendships, family, intimacy. Then there’s SELF-ESTEEM: *achieving mastery, recognition, & respect as a healer * serving as a role model of health for patients & community and finally there’s SELF-ACTUALIZATION: *fulfilling one’s life potential (then helping others do the same). This in my objective in life, not only for myself but for all my patients. I tell them, “I’m just letting you know that I’m not here to put you on an algorithm or to see how we do with your hemoglobin A1C which I’d like to be great, but really my secret reason for being here is that I’m trying to get you to become a self-actualized person. That’s my goal for being here in this medical appointment with you. And a self-actualized person is someone who is fulfilling one’s life potential.” Once you’ve reached that point you are in the perfect position to help others do the same.
And so I think that’s how we need to approach our education. We should not be in medical school environment that’s not conducive to you climbing up this Healer’s Hierarchy of Needs. Obviously this may be a good way to frame things in your life and feel free to add things to it and circulate it around. The thing is there are doctors who feel trapped in jobs they can’t get out of and they are in survival mode. Right? They have no idea and may not have thought about that they’re their employer’s only competition. They’re too busy. That’s why they keep you working full time in a lot of these big offices. I even spoke with the CEO of Oregon Medical Group way back and I asked, “Why don’t you let your doctors work part time? You’d get a lot more out of them when they’re there if they actually got time to spend with their kids, go to baseball games, and do stuff that regular people get to do.” And they’re like, “No we’re not interested in that.” They don’t want part time employees. Why? They don’t want you to have any time for self reflection because you could realize that you don’t belong there. They want you to be in survival mode. Honestly, you’re in paper chains. The minute you realize that you don’t have to be there you can slip right out and get an office like I have for $370 if you’re in primary care. It’s pretty inexpensive in Oregon. Come on. And then you can do magic. You can be the doctor you always wanted. One of the large multi specialty groups in my town lost 18 primary care doctors in one year. Now I don’t think any of them opened their own clinics, but what they might have done is jump into another dungeon somewhere else thinking it might be better in the paper chains at this other place.
You know how many slick ads I get in my mailbox every week promising me $300,000 per year and no call if I go here or there? I wouldn’t trade in what I have for 5 bullion dollars a year. I have a great life. I feel like I’m retired and I’m working! I could make more money working this way if money were my goal. That’s what people ask me sometimes. They just assume that I must be a happy hippie on a hill. You just don’t care about money. Well, that’s not true. I could make more money working this way. On the FAQ that I will send out if you want it just e-mail me and I’ll send it to you. There are doctors who are practicing who’ve opened ideal clinics who are defaulting on their student loans and there are doctors who have opened ideal clinics who are making over $300,000 per year. What’s the difference? One is interested in making over $300,000 per year and one doesn’t really care about money. You can have whatever you want which is why it’s so important for you to figure out what your dream is. Your dream might have nothing to do with making money. After paying off your loans, you just might want to be free and do whatever you want, you know, and live a voluntary simplicity lifestyle. Or you might want to rake it in. You can do that ethically if you set your clinic up properly and you want to work more of a full-time schedule in an ideal medical clinic. You could make far more than any other family practice doctor in the country if you wanted to do that. Some people think: I’ll do that after I pay off my student loans. Let me put my life on hold again for another 5 or 10 years. Maybe later I’ll do something that I really want to do. When I retire I could finally go to Hawaii. You should be able to have fun now. Do you know the zen poet quote? I LOVE that quote!!
That is what I want you to have! Which you can have at any time you decide. Questions?
Question: What is your weekly schedule like? Do you structure your schedule around what you are wanting to do in your life? Or do you have more of a 9-to-5 schedule?
Dr. Wible: Oh no. I’m not a 9-to-5 person. What I call my full-time, part-time schedule (like if I really max out my part-time schedule) I see 8 patients per day 3 half days per week. And I work starting at 2 to 3 in the afternoon because I like to sleep in. I haven’t set an alarm clock in 10 years for work and I really like that. It feels better after all those years of loud noises and things waking you up in the middle of the night in medical school and residency. It’s really great. Before I developed a little bit of a knee issue, I would ride my bike to work and I’d give my patients gifts for riding their bike to the clinic and I’d see them all with their bike helmets on we all kind of rode together. I use to get up in the morning when I was first starting out and go to this coffee shop down the street and do all my patient charts. This is really funny: because I know my patients really well and I schedule them for the amount of time they need. They don’t do online scheduling. I mean, I schedule them through e-mail so it’s not like they schedule themselves. So I know who’s coming in and because I’ve communicated with them, I know what they’re coming in for so I did this as an experiment: I arranged their charts for the day and I would start writing their chart note before they even came in and just to see if I was on track with what I thought was going on and I’d even put down their diagnosis codes and literally when I’d see them I was already done with their chart note before they came in because that’s how well I know my patients. I would, of course, add to the note. When practicing this way, there’s no surprises and “Oh by the way, I have chest pain.” When you have 30 to 60 minutes everything is out in the open at the beginning and you can tell if they are hiding something or if they start crying you can dive into other areas they had not planned to discuss. Does that help?
Question: How many patients do you have total?
Dr. Wible: About 500 patients. If I was working a full schedule (4 full days per week) I could probably take care of 1500 patients well. Maybe see 8-10 patients per day. People who select to come to you when you’re in an office like this which is functional and really healing are people who really want to get better. You should try sitting in different waiting rooms of clinics around town and you’ll notice some places have a really low energy and high misery level and people don’t seem to be getting better there. They just keep coming back for 10-minute visits. Basically, a patient will fall to the level of dysfunction within a clinic. So if it’s full of doctors who feel trapped, miserable, and are thinking of suicide, the patients are not going to be getting that well there. You’re going to have a patient load that’s bigger and needier and more annoying.
A lot of people can’t believe that I could be on call 24-7 and enjoying that because wouldn’t your patients drive you nuts? You don’t want these people calling you all hours of the day. But in actuality, there’s a concept “tragedy of the commons” that indicates that when people perceive of a resource as scarce, the hoard it. So if physicians have a human shield of 10 employees protecting them from ever having to talk too long to a patient and they have these phone trees and all this things that are barriers that prevent an accessible relationship then you will feel hoards of people who are grabbing and needy and you’ll never feel like you can get away and your patients will get on your nerves, but you created that monster. It’s like your kids would probably act out, they’d be doing drugs and getting into a lot of trouble if you were not an accessible parent. If you are accessible to your partner and your kids, you have a normal relationship, people get along well, and they’re not needy and annoying. Did that help? Anything else? If you have to go, that’s great. But I’m going to stay as long as it takes. Take one of these on your way out if you have to leave. And please share these with people who were not here. . .
Question: I’m a first-year student and I’m not quite sure what specialty I want to go into since I’m so early on in this program. I am interested in surgery and I have this crazy dream that I could do a practice similar to what you’re doing as a surgeon. And I was wondering if you have any surgeons who have done that.
Dr. Wible: Yes! You can! In my teleseminar now I have a dermatologist who is a Mohs surgeon who just quit her job and she’s going to open her own practice in Houston. I don’t know any (general) surgeons who are doing this, but I do know an orthopedist who has his own practice and he makes 20% less than working in this big ortho group, but he’s like the coolest doctor in town and people come by anytime and get an X-ray and he’s like a Marcus Welby family doctor like small-town orthopedist. This guy loves it! There is a peds ENT who does this and obviously psychiatrists can do this really easily because what do you need for psychiatry? You don’t even need a stethoscope. It is very accessible to specialists if you want to set up your life this way. Anything else? Okay I guess I answered everyone’s questions. Take a handout.
Addendum: The first thing that I did when I got home after my presentation at the medical school was Facebook Rhonda. I wrote:
“I spoke about Kaitlyn and then got a standing ovation. I will post video soon. I spoke about you as well and read your writing. And held up Kaitlyn’s book. It was amazing. My first standing ovation! Nothing beats a room full of inspired medical students. 🙂
Rhonda and I became fast friends on May 31, 2014, when she shared Kaitlyn’s story as a comment on my blog Why Physicians Commit Suicide. I phoned her the very next day. She has the strongest North Carolina accent I’ve ever heard! I got used to hearing her voice. In fact, I’d hear something from Rhonda almost daily. (To read our correspondence, please see Physician Suicide Letters—Answered). But this time Rhonda never replied to or “liked” my post. I found out later that while I was inspiring these students, Rhonda Elkins went missing. She was found the next morning. Rhonda died, just like her daughter Kaitlyn, by suicide. I attended her funeral yesterday in Clarkton, North Carolina, where I met her kind family and dearest friends. I lost one of the sweetest people I never met. Rhonda, you touched me so deeply. Yet I could only touch your casket. Rest in peace sweet, sweet soul. I’ll continue where you left off with more devotion than ever. I’m here if you need me. XOXO.
My TEDMED talk featuring Kaitlyn Elkins:
Pamela Wible, M.D., is a family physician in Oregon who is devoted to stopping medical student and physician suicides. She offers retreatsfor premeds, medical students, doctors, and others who need help. Watch her TEDx talk on physician suicide. Please read Physician Suicide Letters—Answered to really understand the hazards of current medical education & practice.

 Dr. Wible: Welcome to Physician Suicide 101: Secrets, Lies & Solutions.
Dr. Wible: Welcome to Physician Suicide 101: Secrets, Lies & Solutions. I’m a family physician born into a family of physicians. My parents warned me not to pursue medicine. So I went to medical school. Ten years later, I’m unhappy with the direction of my profession (and I’m not the only one). Then I get this crazy idea: what if I ask for help? Not from the profession that wounded me. Just from random people on the street. So I hold a town meeting and ask patients to help me—design an ideal medical clinic. I promise do whatever they want as long as it’s basically legal. That’s going out on a limb.
I’m a family physician born into a family of physicians. My parents warned me not to pursue medicine. So I went to medical school. Ten years later, I’m unhappy with the direction of my profession (and I’m not the only one). Then I get this crazy idea: what if I ask for help? Not from the profession that wounded me. Just from random people on the street. So I hold a town meeting and ask patients to help me—design an ideal medical clinic. I promise do whatever they want as long as it’s basically legal. That’s going out on a limb.
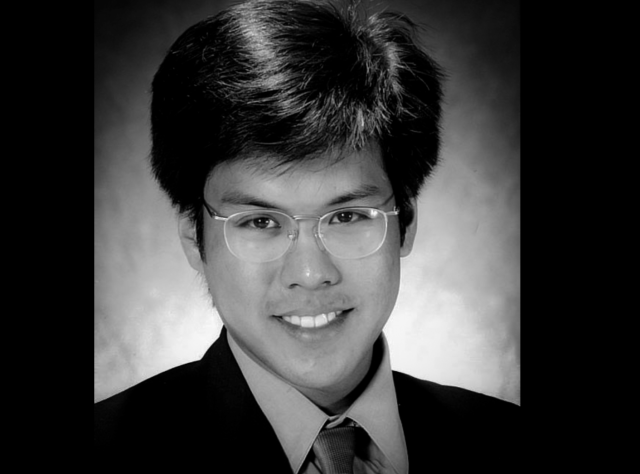
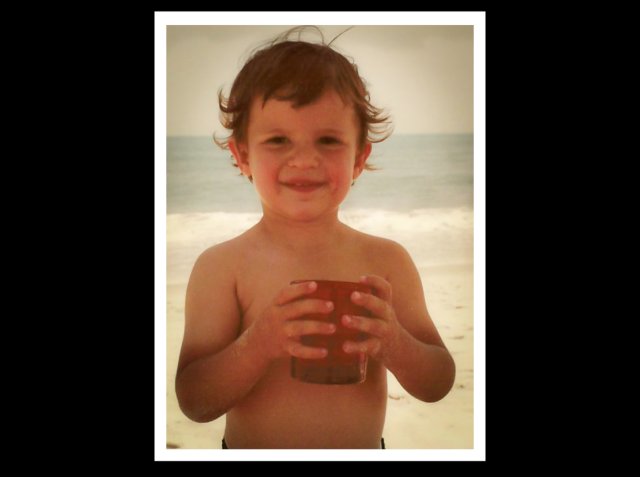





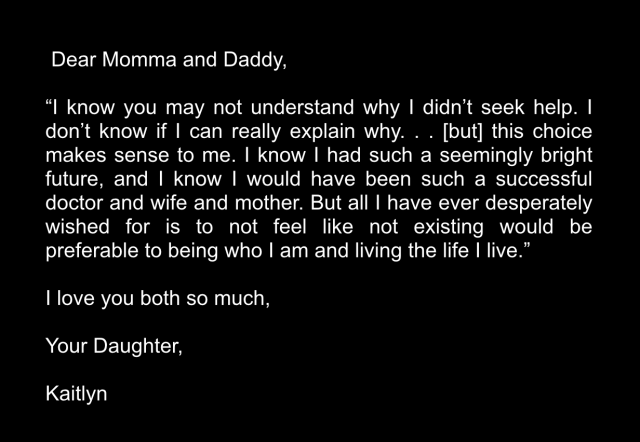



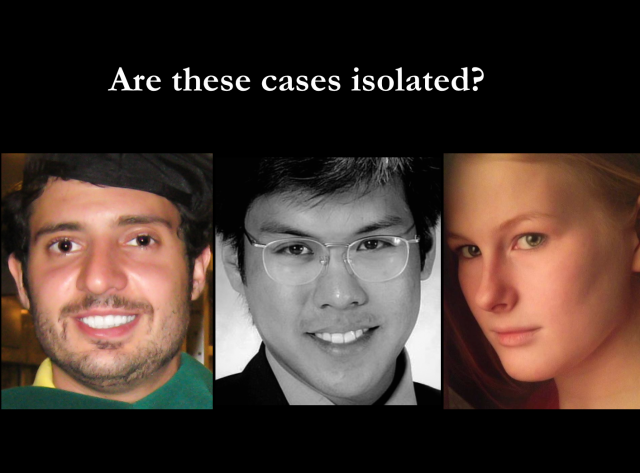
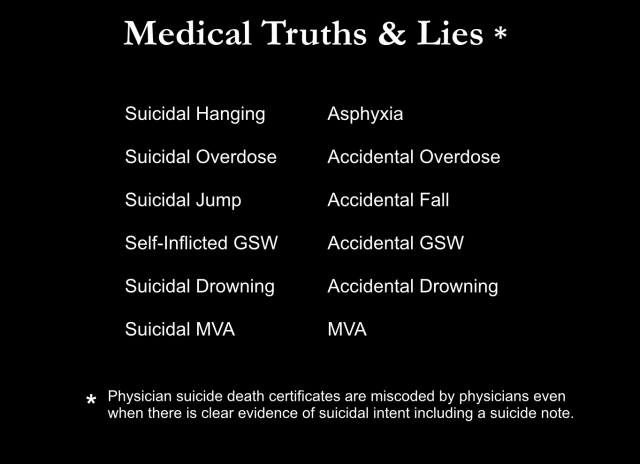


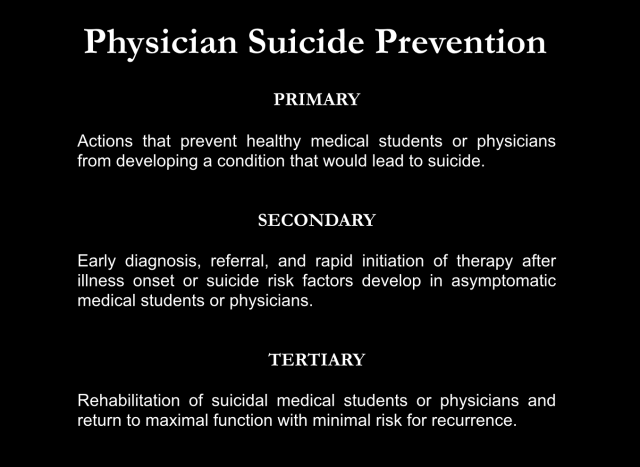
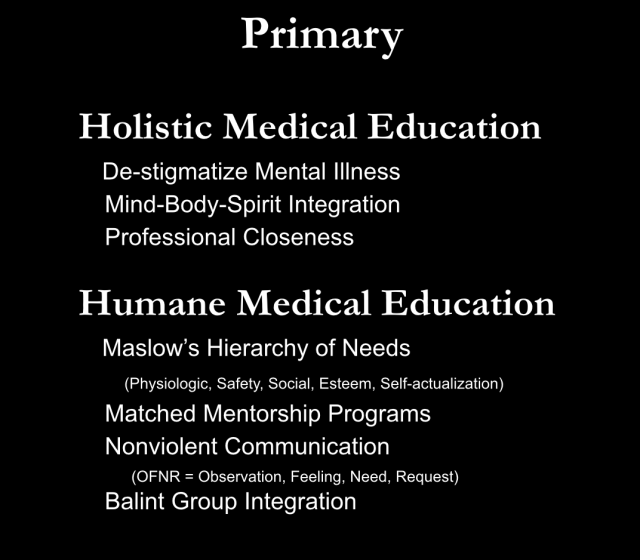
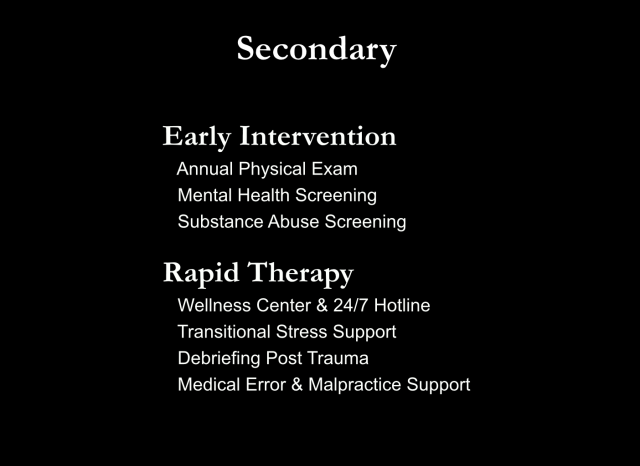



 Pamela Wible, M.D., pioneered the first ideal clinic designed entirely by patients—the original “Patient Centered Medical Home.” She was once a suicidal doctor and now dedicates her life to helping medical students and doctors who are disgusted with, depressed by, and feeling suicidal about their once-beloved careers in medicine. There is hope! Come to the next
Pamela Wible, M.D., pioneered the first ideal clinic designed entirely by patients—the original “Patient Centered Medical Home.” She was once a suicidal doctor and now dedicates her life to helping medical students and doctors who are disgusted with, depressed by, and feeling suicidal about their once-beloved careers in medicine. There is hope! Come to the next 


 A psychiatrist in my
A psychiatrist in my 
 I’m going to read a letter that Kaitlyn’s mother, Rhonda Elkins, wrote. (to read Kaitlyn’s suicide letter and the suicide letters of other medical students and physicians, please see
I’m going to read a letter that Kaitlyn’s mother, Rhonda Elkins, wrote. (to read Kaitlyn’s suicide letter and the suicide letters of other medical students and physicians, please see 
















{kind=link}