
On February, 26, 2015, Pamela Wible, M.D., was named the 2015 Women Leader in Medicine by the American Medical Student Association in Washington D.C. Dr. Wible was nominated by American premedical and medical students as one of the most inspiring women educators in medicine today. Her acceptance speech is filmed and fully transcribed below.
INTRODUCTION: Pamela Wible, M.D., is a family physician born into a family of physicians. In 2004, fed up with assembly-line medicine, Dr. Wible held town hall meetings where she invited citizens to design their very own ideal clinic. Open since 2005, Wible’s innovative model has sparked a populist movement that has inspired Americans to create ideal clinics and hospitals nationwide.
Pamela Wible’s model is now taught in medical schools and undergraduate medical humanities courses and is featured in the Harvard School of Public Health’s newest edition of Renegotiating Health Care: Resolving Conflict to Build Collaboration, a textbook examining major trends with the potential to change the dynamics of health care. Dr. Wible is also the author of Amazon’s top-rated Pet Goats & Pap Smears: 101 Medical Adventures to Open Your Heart & Mind—a book that I had the pleasure of reading and being inspired by a year ago.
When not treating patients in her community clinic, Dr. Wible devotes her time to medical student and physician suicide prevention. Dr. Wible’s work in this area was a huge component of why I nominated her for this award. I truly believe that the conversation that Dr. Wible is beginning about suicide prevention is turning the light toward medical students to reexamine their own wellness as well as the wellness that we provide our peers.
A graduate of Wellesley College, University of Texas Medical Branch at Galveston, and the University of Arizona Department of Family & Community Medicine, Dr. Wible is now called to help students and physicians deliver ideal care to their communities. It is such an honor to introduce Dr. Pamela Wible, an inspiring leader and educator of the next generation of physicians as the 2015 Women Leaders in Medicine Award winner.
* * *
Well, I like to start with my favorite quote. A zen poet once said, “A person who is a master in the art of living makes little distinction between their work and their play, their labor and their leisure, their mind and their body, their education and their recreation, their love and their religion. They hardly know which is which and simply pursue their vision of excellence and grace, whatever they do, leaving others to decide whether they are working or playing. To them, they are always doing both.”
Medicine is an apprenticeship profession. We learn to be doctors—by studying doctors. And patients learn by studying us. The word doctor means teacher. But what are we teaching? If doctors are victims, patients (and medical students) learn to be victims. If doctors are discouraged, patients (and medical students) learn to be discouraged. If we want happy, healthy patients, we must fill our clinics & hospitals with happy, healthy doctors.
But when I look around, I really don’t see many happy doctors. So my mentors are—medical students. I love your youthful joy and exuberance and I’m inspired by your endless curiosity and conviction and compassion. I want to grow up to be just like YOU.
I want to be like Becky, she’s a medical student in Oklahoma. She has a dream of providing care to the poorest of the poor of Oklahoma City. And I want to be like Julia, a med student I met in New Jersey. She wants to open her clinic on an organic farm. And I want to be like Sasha, a premedical student from Pennsylvania who wants to “cry with and love on” her patients. I am inspired to be the best version of myself when I think of these people and when I think of medical students and the joy and love that they have and the desire that they have to serve people when they enter medical school. And so I want to keep that joy alive for the rest of your medical career. And I want to bring that joy back to my colleagues who have lost this.
I’m a family physician in Oregon and I love my patients. I hug them and kiss them, and I do housecalls. And they all have my home phone number. I’m on call 24/7. That would seem like a hardship, but it’s not. I never really feel like I’m working. I think that’s because I’m self-employed—which is how most doctors worked until very recently. For centuries physicians have been self-employed.
One reason why I like being self-employed is that I haven’t had to set an alarm clock in 10 years for work. Because I work afternoons and evenings 3 half-days per week and it’s AWESOME! I highly recommend it. And I like being self-employed because I’ve never turned anyone away for lack of money. Because I’m the boss and I can do that. And I like the boss. Being self-employed I have a lot of fun. I can break the rules that don’t make sense because I’m self-employed. And here are 3 rules that don’t make sense and I would encourage you all not to follow these 3 “rules” in our profession:
1) I refuse to practice professional distance. Because what patients really want is professional closeness.
2) I refuse to practice cookbook medicine. Because patients aren’t chocolate chip cookies. I’m not a cookie cutter doctor—and neither are you.
3) I refuse to practice assembly-line medicine. Because I didn’t go to medical school for all these years to be a turned into a factory worker—and neither did you. Patients aren’t looking for a factory worker or a zombie robot. They are looking for a real human being so I would encourage you to stay real during your training. You’re going to be a lot happier that way.
The other thing about breaking away from assembly-line medicine as was discussed during my introduction is that I was able to create a new model with the help of my community. I basically had a town hall meeting where I told everyone that my job sucked and that I was suicidal and that if they didn’t come up with a better way [for me to practice medicine] I was just going to be a waitress or something. I just could not see continuing practicing medicine in this insane corporate assembly-line 7-minute-visit practice style so I collected 100 pages of written testimony. I pretty much told them I would do whatever they wanted as long as it was basically legal. So if you could just tell me what’s your dream. Write my job description for me if you wouldn’t mind because it’s not really working for administrators to write my job description. I’d rather work for the people themselves. And I got 100 pages of testimony and was able to adopt 90% of what patients needed in my town and we were open one month later! It’s not rocket science. You don’t really need to wait for the government to do this for you.
Buckminster Fuller has a quote I really like. “You never change things by fighting the existing reality. To change something, build a new model [ideal medical care] that makes the existing model [assembly-line medicine] obsolete.” I hope you’ll join the movement for ideal medical care and that YOU will be the change you want to see in medicine.
“A dysfunctional medical system can only exist on the backs of a disempowered physician population—the precursor of which is an abused medical student population.”
So I hope during medical school you will break the rules when need be and that you won’t be too well-behaved. And that you will stand up against intimidation, bullying, and abuse because it doesn’t get better. You might as well stand up at the beginning.
We need to take our profession back. And if you need any help feel free to Facebook me, be my friend, email me, call me anytime. My home phone number is 541-345-2437. Put it on speed dial in case you are bullied or abused. I am accessible. In case you want to know sooner than later what to do, come to my talk on Saturday. I’m giving a talk on some strategies that you can use to confront unethical behavior in medical school with grace and success.
“The truth is: it’s impossible to be a victim and a healer at the same time. So I hope you’ll choose being a healer rather than a victim.”
And I thought I’d read this most beautiful chapter that came out of a series of interviews with doctors called The Raw Truth. This is the reason why I became a doctor and I think it is why many of us became doctors.
I often wonder: Why am I a doctor?
I want to live in the real world, a world without pretense, a world where people can’t hide behind money or status. Illness uncovers our authenticity. Doctoring satiates my need to be witnessed and to witness the raw, uncensored human experience. I crave intensity.
Like an emotional bungee jumper, I live to inhale the last words of a dying man, to hear the first cry of a newborn baby, to feel the slippery soft skin in my hands, to cut the cord and watch a drop of blood fall on my shoe, to wipe a new mother’s tears, to introduce a father to his son, to hold a daughter’s hand as she kisses her father good-bye one last time.
I am a doctor because I refuse to be numb. I want to live on the precipice of the underworld, the afterworld, to look into patients’ eyes, to free-fall into an abyss of love, despair, death and then wake up tomorrow and do it all again.
Maybe doctoring fills a hole, a void. I doctor for connection, to be needed—to be loved.
Chapter 90, The Raw Truth, Pet Goats & Pap Smears.
And in summary, at its core, doctoring is intimacy and intimacy means “in-to-me-see.” It’s when we see so deeply into another, that we find our own reflections and discover ourselves. So I’d like to ask you to be a healer and not a factory worker. And I’d like to ask you to take your eyes off your computer and look into your patients. Because it’s there [in your patients’ eyes] that you will find the truth and discover yourself and your path in medicine. Thank you.
* * *
Dr. Wible’s Q & A went on for 2 hours after her acceptance speech. Here are some of the medical students and physicians who hung out with her until nearly midnight:

Need a speaker at your next event? Contact Dr. Pamela Wible to speak at your grand rounds, medical conferences, and medical school commencement ceremonies.

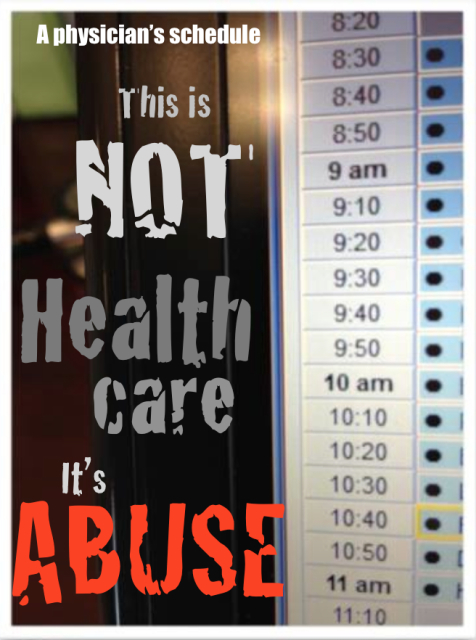 A physician in Texas posts this photo on Facebook. Caption: “My schedule one morning in January 2014. Never again . . .”
A physician in Texas posts this photo on Facebook. Caption: “My schedule one morning in January 2014. Never again . . .”













