Hi Pamela,
I’m a medical student in the UK. Though I’ve only been in med school since September, it has already taken its toll on me. Before I started I was so in touch with my emotions, spirituality, and nature. Now I feel so empty and desensitized. I hate that when faced with the horrible circumstances of another person, I just don’t feel anything anymore. How can I overcome this? I so badly want to tap into the vibrant me from 6 months ago!
Before starting medical school, I was a curious and loving young man. My life hadn’t been plain-sailing: I had been through my parents’ divorce as a young teenager; I had suffered bullying in a hostile school environment, and I had come out of the closet as gay. All of these things sound quite monumental for a young person to go through, but nothing prepared me for the agony of medical school. You see, when my parents divorced, I was sad, I cried, I grieved for the family life I would no longer have, and I recovered. When I was bullied at school, I was hurt and upset, but knew they were wrong which gave me strength. And when I came out of the closet, I was bursting with emotion: of anticipation, excitement, terror. All of these experiences were by no means pleasurable, but I FELT them, and that’s what made me feel alive. They were painful, but they illuminated the happy times in my life and made me a stronger and more empathetic person as a result. I looked into people’s eyes and could sense their pain a little more because of my own personal experiences, and enjoyed feeling connected to their lives. I was spiritual. I would pray and meditate and marvel at the beauty of nature and humanity around me. I was genuinely excited for my life, the people I might help. I wanted to be intimate with people, rejoice in their success, and feel the pain of their sorrow.
Then I entered medicine.
From the first few days, I could tell something wasn’t right. I entered this profession with the intention of becoming a healer, yet, when I looked at my lecturers, I mainly saw didactic scientists, not healers. I looked around me and saw egotistical, power-hungry students. Many were concerned with status, competitive to the extent that they all wanted to outdrink each other on boozy nights out and have the most sex out of our whole group. They wanted to be the best at everything: in their exams, and in their personal lives. Yet no student has ever spoken with genuine concern and feeling for patients. When I organized a talk by two individuals suffering from HIV, hardly any of our class turned up—I’m talking about 2-3% of the students. When I asked some why they did not attend, many just didn’t care. “We don’t need to know it for our exams,” one said. “I don’t think I’d get anything from it,” smirked another. I was aghast by how little they cared.
At this point, I really questioned the establishment of which I was becoming part. Even with the brightest soul and the best will in the world, it is hard to survive in an environment at complete odds with our own intentions. This soon took its toll on me. I felt like I was in a constant battle to retain my care, my love, my empathy. But I feel like I am losing.
While the challenges in my life were at times very painful, medicine has caused me to feel something I never imagined could be so bleak—nothingness. It is quite astounding actually how little I feel nowadays. I have lost my libido (In fact, I have been convinced I was asexual for a time), and I feel numb on a daily basis, like a nurse has injected some local anesthetic into my heart which hasn’t worn off. Nothing seems to bother me anymore. After cadaveric dissection, nothing is gruesome, the boundaries by which I could operate on someone without feeling any hesitation are endless. There’s something about hammering a ribcage open with a chisel on a deceased old lady that breaks down those barriers for you, and they can never be built back up. In addition, disease and death are talked and laughed about in such matter-of-fact ways that they’ve become boringly dull to me. No longer am I heartbroken for the cancer patient, or devastated for the young mother who died in a car accident, because I feel nothingness. We are only ever taught about the scientific basis of afflictions, never the emotional or spiritual impact on both the patient—and ourselves.
My spiritual life has suffered too. No longer do I appreciate the world around me with the overflowing gratitude I used to hold. Instead, I just wallow. I am strongly considering dropping out of medical school to pursue another path, not because I detest the vocation, but because I am scared I am losing pieces of me that I will never get back. I am scared that after only 6 months, I am just a vessel with no life and that I will never feel what it feels like to feel ever again. I am scared I will never have another tear fall from my eye. Is really worth sacrificing my soul to this profession? I feel ripped apart.
Please let me know if there are any ways to cope with this torturous predicament.
With much love, even though it is so hard to gather from a numbed heart,
Luke
* * *
Luke,
Join our teleseminar this Sunday (scholarships available for med students)
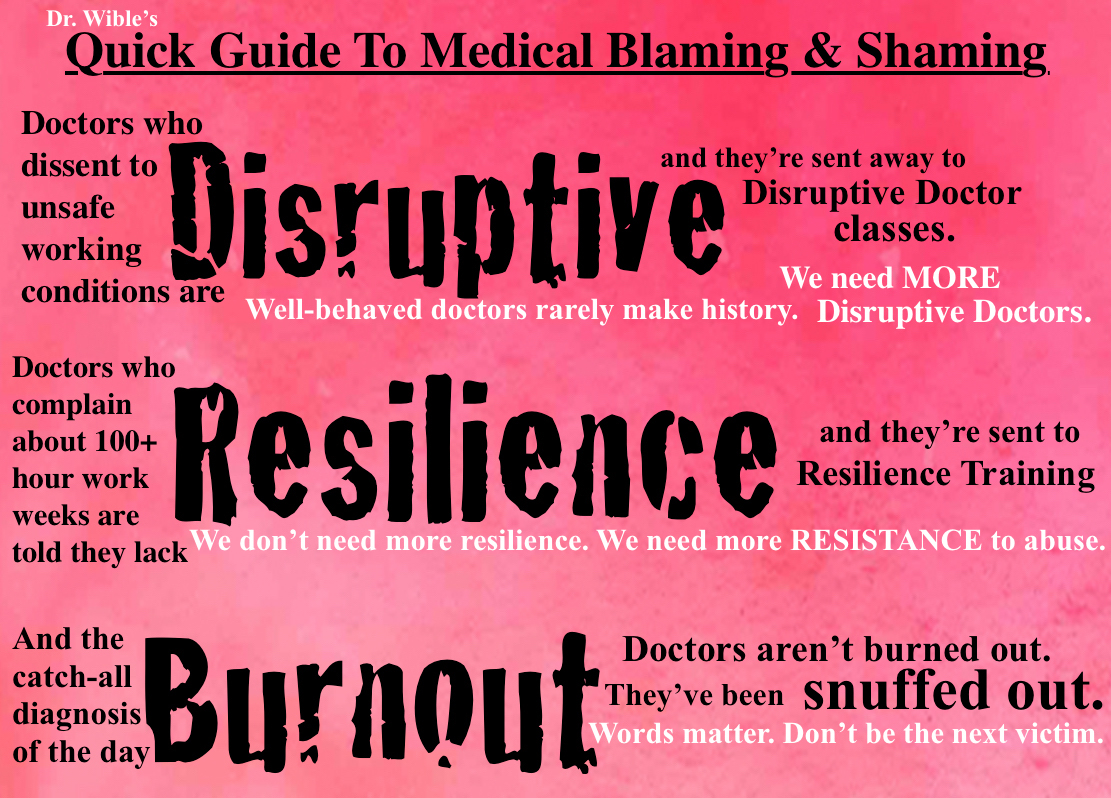
You are not alone. Med students all across the world experience the dehumanizing effects of medical training. The basis of our education is a flawed reductionist medical model that views the human body as a machine—a bag of parts to be conquered. Reductionism (the opposite of holistic medicine) leads to mind-body-spirit disintegration. Consequently, you are losing connection with your heart and soul—the reason you went into medicine—the purpose of your very life.
Loss of meaning, loss of self, leads to pain. Pain leads to self-medication with alcohol, drugs, sex—anything to numb oneself and distract from the loss of soul. Sustained numbing leads to permanent numbing and an inability to connect with oneself or others.
What can you do to overcome your loss of self? My best advice:
1) Keep a clear and unwavering focus on your dream—the original vision that led you to medicine. Read your personal statement daily. Hang it all around your house. Never allow anyone to steal your dream.
2) Surround yourself with inspiring mentors—other physicians who are living their dreams in medicine. They will guide you in the right direction. Avoid advice from cynics and naysayers for they are wounded too. I will totally get you into our mentorship group. Contact me here.
3) Maintain your physical health. Exercise, eat well, sleep. Balance your intellectual pursuits with time to relax and be INSIDE your body. I highly recommend weekly massage to help you remain present with yourself. The benefits are not just physical. To care for others, you must first care for yourself. Massage is a great way to learn how to receive care and to form a therapeutic relationship with a trusted healer who can help you through medical school.
4) Maintain your emotional health. I believe all medical students should receive weekly counseling with a professional (not a friend, not a spouse). If you feel sad, cry. Tears are cleansing. When humans bottle up their trauma with no outlet, they become numb, detached, sick.
5) Maintain your spiritual health. Whether you meet with your church pastor or meditate at an altar in your home, devote time at regular daily or weekly intervals to spiritual self-care or you will lose connection with your soul.
6) You must be well to guide others to health. By caring for yourself, you will not only help patients; you’ll help your classmates and teachers heal. They are wounded too. Be a beacon of hope for them. Even if triggered by your joy, they’ll be less likely to injure you with their pain. They need you.
7) When you are resourced and well, you will once again be able to look into people’s eyes and be a sacred witness to their suffering. You will experience true intimacy which means “in to me see.” For patients to see inside you, and for you to see inside them, you must be inside your body.
Blessings to you on your journey . . .
Love,
Pamela
Want to heal your soul? Attend our next retreat!
* * *
Pamela Wible, M.D., was named one of the 2015 Women Leaders in Medicine by the American Medical Student Association. Dr. Wible is the author Physician Suicide Letters—Answered. Need a letter answered? Contact Dr. Wible.