Please stop using the word burnout. You’re not burned out. You’ve been abused. Let’s get the diagnosis right.
We enter medicine as inspired, intelligent, compassionate humanitarians. Soon we’re cynical and exhausted. How did all these totally amazing and high-functioning people get screwed up so fast? ATTENTION medical students and doctors: It’s NOT your fault.
“Burnout” is physical and mental collapse caused by overwork.
So why blame the victims?
Victim blaming and shaming, bullying and hazing, all lead to increased suicides.
The fact is medical students and physicians are collapsing because they are suffering from acute on chronic abuse. At some medical schools, 100% of students report abuse. Do you think this gets better? Abused medical students become abused doctors who may one day abuse patients. Human rights abuses are commonplace in our hospitals, clinics, and medical schools. This doctor worked 7 days in a row with almost no sleep!
Think abuse is too strong? Read the UN Declaration of Human Rights. Countries get in big trouble for this sort of behavior. So why is it okay for our health care institutions to perpetrate human rights abuses on their own students and employees? It’s not.
Think the doctor below is burned out? Nope. She has been ABUSED!!
Docs, stop playing nice. You are being abused.
Only you can stop this crap.
How do you know if you’re being abused at work? 1) You don’t get lunch or bathroom breaks. 2) You are forced to work multiple-day shifts. 3) You are not allowed to sleep. 4) You are forced to see unsafe numbers of patients. 5) You can never seem to find “work-life balance.” 6) You are threatened verbally, financially—even physically. 7) You are bullied. 8) And if you ask for help, you’re called a slacker or worse.
If any of this sounds familiar, it’s NOT YOUR FAULT.
YOU ARE A VICTIM OF ABUSE.
So what should you do? Sign up for a resiliency training? Meditate? Take deep breaths? Your goal should NOT be to cope with abuse. Your goal should be to STOP it.
Burnout blames the victim, not the perpetrator. It implies that YOU are to blame, not the system, not the perpetrators of the mistreatment.
To treat burnout, health care institutions may offer resiliency classes to train doctors to prioritize self-care and manage their emotions. WARNING: You can not meditate your way out of abuse. Taking deep breaths will not end your abuse.
WHAT YOU MUST DO: If you are being abused, YOU MUST LEAVE YOUR ABUSER. I know it’s scary. You are not alone. Need help with your escape? I’ll help you. Contact me.
Remember: YOU were born to be a healer, not a victim.
Please break the cycle of health care abuse that leads to suicide among doctors and poor care for patients.
Pamela Wible, M.D., founded the Ideal Medical Care Movement. She helps doctors open their ideal clinics through her popular teleseminars & retreats. When not caring for patients, she devotes her life to eradicating health care abuse. Videos by TEDMED and GeVe.
Yesterday I spoke with 500 medical educators who are responsible for educating more than 26,000 medical students across 44 medical school campuses in the United States. Before my presentation, I asked 500 medical students: What are 3 things you’d like to tell your dean (but are afraid to say)? I’ll do it for you.
Here’s the basic message I delivered to a room full of medical school deans, provosts, presidents, and administrators in my keynote, Humanizing Medical Education: How To grow A Happy Doctor.
Isn’t it amazing that we know how to perform lung transplants, map the humane genome, grow organs in laboratories, but we don’t know how to grow a happy doctor? We do know how to grow unhappy doctors. Here’s what a medical student named Sam wants you to know:
1) Med school is the single most unhealthy thing I have ever done for my body, mind, and spirit.
2) I was on zero psychiatric medications and now I am on more than one, and it’s my second year of med school.
3) The only communication the administration has with us is through fear mongering and the upperclassmen just tell us to get through it and it’ll be over soon.
I’ve heard from lots of medical students like Sam. So I synthesized all the responses I received from students into the top 10 commandments for medical school educators. Yes, this is what medical students want to tell you but are afraid to say.
The 10 Commandments for Medical Educators
1) Teach leadership, transformation and empowerment in the curriculum. Empower me so I can empower patients.
2) Stop creating an environment that encourages competition among students.
3) Tell me that it’s okay to cry in front of patients if it’s on their behalf.
4) Ask what inspires me and ask how you can help me achieve my goals.
5) Respect us as adult learners. Avoid condescension. Don’t revel in our ignorance. We want to learn. Try not to kill our curiosity.
6) Advocate for humane treatment of attendings. So many docs have Stockholm syndrome, and see themselves as strong and capable, while seeing med students as whiny lazy kids who need to grow thicker skin. They need to be cared for and educated so that they see themselves as survivors of abuse—and empowered to break the cycle of abuse.
7) Be more concerned about your students wellbeing than damn Step 1 scores.
8) Provide emotional support for doctors and med students. Our wellbeing benefits the whole system. We are not the enemies here.
9) Please don’t train me to forsake my humanity to be a better doctor. My humanity should be celebrated, enhanced, and matured, not demeaned, degraded, or insulted.
10) Show me empathy.
What happens when medical training fails to follow the sage advice of these students? More of this:
Pamela Wible, M.D., is a family physician who is determined to stop the medical culture of bullying, hazing, and abuse that has injured countless medical students, physicians, and patients. Want to help? Contact Dr. Wible.
Pamela Wible, M.D., takes on physician suicide in her TEDMED talk (delivered on November 18, 2015 and now released to the public on March 23, 2016). Learn more about Dr. Wible and her talk at TEDMED.com. Full transcription below:
I love the three things that people fear the most: death, disease, and public speaking. Here’s how it all started. At four, I was so talkative (and bossy) no babysitter would stay with me. So I tagged along with Mom, a hospital psychiatrist, interviewing suicidal patients. Then she’d drop me off at the morgue with Dad, a pathologist. He’d open these big cooler doors and say, “Good morning! Is anyone home?” then introduce me to his patients as a “doctor in training” and leave me there talking. My first captive audience!
Now I’m a doctor and I’m speaking on behalf of thousands of doctors who couldn’t be with us. But they’re here in spirit. I simply ask that you open your heart to their words . . .
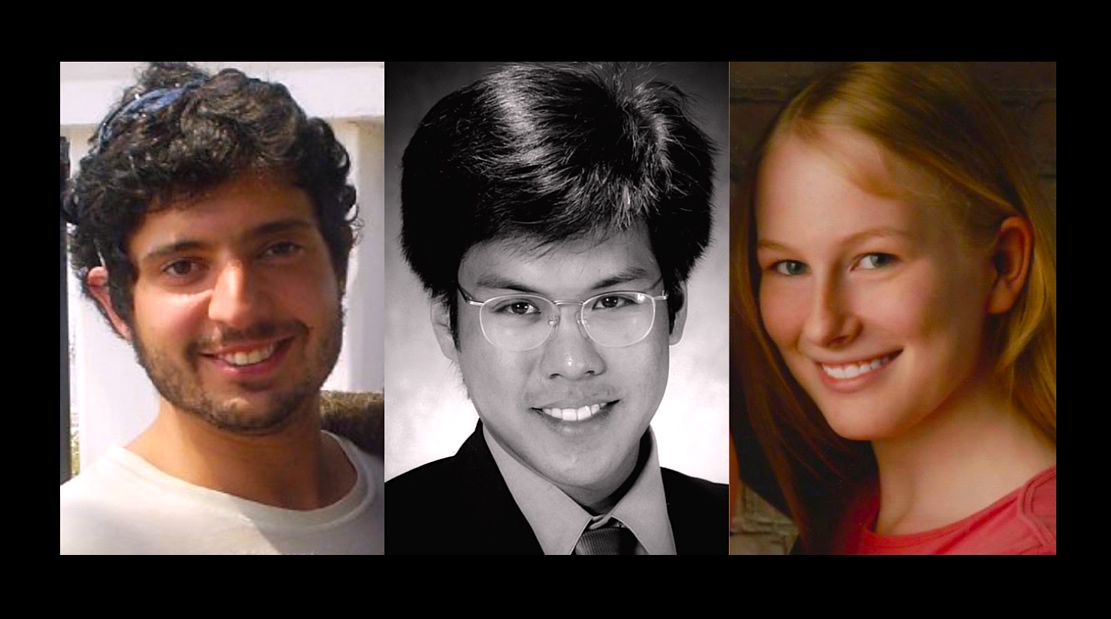
“Dear Momma and Daddy, I know you may not understand why I didn’t seek help, but this choice makes sense to me. I know I would have been such a successful doctor and wife and mother. I love you so much, Your daughter, Kaitlyn.” Date of death: April 11, 2013. Cause of death: asphyxiation by helium inhalation due to untreated depression in medical school.
Each year more than one million Americans lose their doctors to suicide.
Across the country, our doctors are jumping from hospital rooftops, overdosing in call rooms, found hanging in hospital chapels. It’s medicine’s dirty secret. And it’s covered up by our hospitals, clinics, and medical schools.
No medical school wants to be known as the suicide school. No hospital wants to be #1 for interns jumping from rooftops. No one wants to become a doctor—to kill themselves. It’s the ultimate oxymoron: the barefoot shoemaker, the starving chef, the suicidal doctor.
So why? What the hell is going on? And why is this such a secret? And why am I piecing this together between patients? I’m a solo family doc, yet somehow I’ve become an investigative reporter, a specialist in physician suicide. Why? Mostly because I can’t stop asking why. Why both doctors I dated in med school died by suicide. Why eight doctors killed themselves—just in my sweet little town. So I keep talking and writing—and listening for the truth. And because I’m listening with my heart and soul 24/7, my cell phone has turned into a suicide hotline and I’ve received hundreds of letters from suicidal physicians.
You may be wondering: why do so many people “who want to help people” kill themselves?
Anna, a retired surgeon writes, “Dear Pamela, I was happy, secure, and mostly unafraid until med school. I recall in vivid detail the first orientation day. Our anatomy professor stood before an auditorium filled with 125 eager, nervous, idealistic would-be healers and said these words: ‘If you decide to commit suicide, do it right so you do not become a burden to society.’ He then described in anatomical detail how to commit suicide.”
What better way to bring shame to your alma mater than with a failed suicide. Alma mater means “kind mother,” yet doctors describe med school as “a soul-crushing boot camp, a dehumanizing nightmare, my own personal Vietnam.” Medical training is neither motherly nor kind.
“I love you mom. I’m sorry. Vincent.” Date of death: August 25, 1998. Cause of death: asphyxiation by hanging due to bullying, hazing, and sleep deprivation as an intern at a New York hospital.
Sleep deprivation is a torture technique. Fear as a teaching tool just teaches us to be afraid. I can help doctors, though there’s one group I can’t help—patients. From all over the country they write me, begging me to find them caring doctors. How can we give them the care we’ve never received?
“Dear Pamela, I definitely graduated med school with PTSD. It has changed me forever. I will never be the same again. We had two suicides and one murder, skull crushed with a bat, and another serving life in prison for murdering a classmate during a delusional episode after not sleeping for a month. Please change medical education. We were so beaten down. It takes a lot for me to cry but I cried all the time along with everyone else, but we hid it from each other, of course.”
Fact: we enter medicine with our mental health on par with or better than our peers. Suicide is an occupational hazard of our profession.
Photo credit Jerod Harris for TEDMED
“Dear Some, My family, I love you. To others who have been good friends, I love you too. This is just the end of the line for my particular train. Earth wasn’t a great place for me. We’ll see what else is out there. Will miss you all! I’m sorry for what it’s worth. Love Greg.” Date of death: June 22, 2012. Cause of death: Hemorrhage by transection of the arteries to his wrists and ankles. Okay so what happened here? Greg died just hours after being told not to follow his psychiatrist’s safety plan. By whom? By an agency (with no physician oversight) that controlled his medical license.
Our medical schools, clinics, hospitals (and related “agencies”) actually cause mental health conditions in doctors, then they blame us and force us to release our confidential medical records. And in the end, they take our license. But it gets worse . . .
“Dear Pamela, Do you know what really hurts? The fact that anyone can look me up on the Internet and read my dirty laundry. I’m publicly shamed, punished for being ill. I will only know peace when I am gone.”
Maybe that’s why my friend, an excellent psychiatrist, drives 200 miles out of town, pays cash, and uses a fake name to get mental health care.
“Dear Pamela, You don’t know how thankful I am for your article on physician suicide. I wanted to hug you after reading it. I had a really rough day—130 outpatients, sixty emergency admissions in a twelve-hour shift. I’m a final year internal medicine resident in one of the busiest hospital in India. Two patients on each bed, two lying together on the floor. Poverty, misery, pain all around. I’ve declared twelve patients dead in a day. I just don’t feel death anymore, just don’t feel human. My uncle died recently, I felt nothing. This profession demands too much from us. I’ve thought of suicide a thousand times. The misery is too much for me. . .”
I’m a perpetual optimist, yet after a decade of seven-minute visits at assembly-line clinics, even I felt suicidal. I thought I was the only one.
Then I got this crazy idea. What if I ask for help? Not from the profession that wounded me. So I asked patients: “What is ideal health care? What kind of doctor do you want?” They told me an ideal doctor is happy, has a big heart and a great love for people and service and an ideal clinic is a sanctuary, a safe place, a place of wisdom with fun flannel gowns, complimentary massage while waiting, where nobody is turned away for lack of money. I followed their instructions—and opened their ideal clinic—the first clinic designed entirely by patients!
Photo credit Sandy Huffaker for TEDMED
My life is like a lovefest now! My patients and I have inspired hundreds of doctors all across the country to open ideal clinics. At times I feel like the happiest doctor in America—until I get yet another call about a suicide or I read a letter like this:
“Dear Dr. Wible, I’m a patient who just got home from another insulting, degrading appointment with my doctor. I’m literally crying as I write to you. . .”
I call her. She shares her horror story. I share mine. She never knew doctors could be suicidal. She never knew she could be the victim in a cycle of abuse that began on day one of med school when her “insulting” doctor was still an idealistic student. How could she know that abused medical students become abused doctors who may one day abuse patients?
So how do we stop institutional abuse? Physician suicide hotlines inside our hospitals? Resilience training for our wiped-out doctors? Meditation classes for medical students? Wait, is our goal to help victims cope with abuse? Or to end the abuse?
It’s not costly or complicated to stop bullying, hazing, and abuse. It’s been outlawed from elementary schools to fraternities. Why not health care?
Medical culture and education must change. Yet cultures and institutions don’t change because we ask them to change—even when it’s in their self-interest. They change when they’re forced to change.
I favor the honor system. What if those in charge are not behaving honorably? What if our medical system continues to blame, shame, and publicly humiliate its victims?
Maybe it’s time for us to give them a dose of their own medicine. How? By shining an embarrassing public spotlight on physician suicide.
On behalf of those we’ve lost (and those who are barely hanging on), I want to thank you for shining your light into the darkness—because if we all shine our lights together, there’s is no darkness to fear. But mostly I want to thank you for your courage, for following a fearless little four-year-old through the morgue and into the coolers to meet a few of her friends.
Greg Miday, Vincent Uybarreta, Kaitlyn Elkins ~ Rest in peace sweet souls. We miss you.
This week I learned of a third physician who has jumped to her death in NYC. Her colleague writes:
Dear Pamela,
A medical resident died at my apartment building (subsidized housing for hospital employees) yesterday. I must have obliviously walked under her dead body on the scaffolding on my way to work yesterday. I just had an urge to tell someone about it and thought I’d tell you.
There was a “global notification” email to our medical community about the “tragic loss” of a medicine house staff member. My supervising attending told me it was a suicide. My co-resident told me that she heard from the front door man that it was in our building. And then last night I just googled to try to find out more and found this article. The scaffolding has been there for a full year to restore the cement on the outside of the building. Plus there are ropes that go from the roof down to the ground, one of which hangs in front of one of my windows. It has always looked ominous to me and reminded me of a hang rope. There are bars on my windows. State law requires this if a child lives in the apartment. They don’t remove them if the next tenant (like me) doesn’t have a child, so I would expect they’re on all of the windows by now, since this building is decades old. She must have uninstalled the bars or gone to the roof.
There was the death of a student while I was an undergraduate. I could see the building she fell from whenever I looked out the window from the yoga classes at the school gym and it always reminded me of that fall. The university chaplain told me that a friend had convinced her to walk back from the ledge and she lost her footing on the attempted return and fell to her death. That’s the most horrible suicide story I’ve ever heard.
I want to be able to go home without being reminded of suicide. The program directors are going to meet with us, so maybe I’ll learn more about what happened then. I appreciate your offer to talk and I have your phone number in my phone. Thank you!
Anna
I published this letter with Anna’s approval. I commend Anna for her courage to break the silence on physician suicide and for her willingness to reach out for help. Survivors, colleagues, and families all need support after a suicide.
I wrote about the first two doctors who jumped to their deaths in NYC here. Each year, more than one million Americans lose their doctors to suicide. We can prevent the senseless deaths of our compassionate and brilliant young doctors by breaking the silence on physician suicide. Please watch this 2-minute movie trailer and join me in bringing physician suicide out of the darkness and into the light.
Addendum: View documentary film trailer above. Stay tuned for world premiere in NYC in September, 2018. Please listen to FREE audiobook download below (like a 3-hour suicide hotline for doctors and med students).
Pamela Wible, M.D., has dedicated her life to preventing medical student and physician suicide. She is the author of Physician Suicide Letters—Answered.