Pamela Wible, M.D., speaks to 500 medical educators at AACOM (American Association of Colleges of Osteopathic Medicine) on April 7, 2016. Thought provoking & funny. Fully transcribed below: (Note: Video contains scenes from documentary film, DO NO HARM. 2016 Copyright Symon Productions, Inc. All Rights Reserved).
Dr. Stephen Shannon: Good morning, everyone. To continue our deliberations from last night’s presentation by Dr. Aviad Haramati on the theme of this year’s conference and the topic of resilience, it’s my distinct pleasure to introduce this morning’s plenary speaker, Dr. Pamela Wible. She is a board certified family physician who received her medical degree from the University of Texas Medical Branch at Galveston and completed her residency program in family and community medicine at the University of Arizona.
Born into a family of physicians, they warned her not to pursue medicine. She soon discovered why. Quickly disenchanted with the assembly-line model of patient care, instead of giving up on medicine, Dr. Wible decided to reinvent it for herself and for her patients. She held a series of town hall meetings in her hometown of Eugene where she asked people to describe their vision of an ideal medical practice.
Three months later she opened a clinic designed entirely by her community. In her innovative populist-designed practice she now works part-time and sees patients for as long as an hour at a time. Open since 2005, Dr. Wible’s community clinic has inspired others to create ideal clinics and hospitals of their own nationwide.
Her innovative model is now taught in a number of medical schools and featured in Harvard School of Public Health’s newest edition of Renegotiating Health Care, a text examining major trends with the potential to change the dynamics of health care. She speaks widely on health care delivery and is the best-selling author of Pet Goats & Pap Smears and Physician Suicide Letters—Answered.
Dr. Wible has experience in traditional and complementary healing modalities and explores the emotional, spiritual and physical realms of disease with her clients. When not treating patients, Dr. Wible devotes herself to medical student and physician suicide prevention. Many of her articles have been picked up by major news outlets such as NPR and The Washington Post. Her work on physician suicide was the focus of a prime-time segment of America Tonight. She most recently provided a presentation nationally through the TEDMED program in November, which hopefully you all will have had a chance to look at as it was distributed. That program is available to all of our osteopathic medical programs.
An inspiring leader and educator of the next generation of physicians, Dr. Wible has been named one of the 2015 Women Leaders in Medicine by the American Medical Student Association. Please join me in extending a warm AACOM welcome to Dr. Pamela Wible.
Dr. Pamela Wible: Wow! Love all these smiley faces early in the morning. I have a question about last night’s plenary. Who was there? Just raise your hand if you were there. I’m just curious was I the only one that was crying during that talk? Did anyone else have even a tear drop from their eye? Raise your hand. I’m just curious. Mostly women, yeah.
I couldn’t even sleep last night, trying to figure out why was I crying during the meditation (which meant that I really didn’t do very well during the meditation because I was distracted). I think what came to me is that it was just so beautiful to finally be in a room of medical educators, like 500 of us all meditating together for medical student mental health. I didn’t know I was going to witness that in my lifetime. I didn’t see that happening at my medical school of origin in Texas. It was beautiful.
I’m really honored to be here and I feel just a sense of optimism knowing that so many of you are as passionate as I am about medical student mental health. Welcome, officially, to my talk which is more of a conversation. I really don’t want to sit and talk. I would prefer to hear from you all, and there will be a lot of opportunity to interact and to ask questions and such.
The topic is “Humanizing Medical Education: How to Grow a Happy Doctor.” What I thought last night that was so interesting about this (and I didn’t quite get this when I came up with the title) but it’s amazing and actually very incredible what we’ve discovered in modern medicine and what we’re able to do. We can do lung transplants. We can map out the human genome. We can grow organs in laboratories. But we haven’t quite figured out how to grow a happy doctor. Isn’t that interesting how many cool things we can do, but we haven’t quite figured that out? We’ve figured out how to grow an unhappy doctor. We’re really good at that. We’ve figured out how to grow unhappy medical students.
I would like to invite you all to just interact with me from your perspective. It’ll really help me because I’ve heard from the medical student perspective. I hear from patients all the time—the end result of not having happy doctors and medical students. You’re actually a really new crowd for me. I haven’t been able to hang out with medical educators since I was in medical school. I really value your input and your insight into this topic because it’s going to take all of us together to really do a good job with reforming and humanizing medical education.
I want to promise you one thing with my talk today (and our conversation) which is that by the time you leave here you’re going to have at least 2 to 3 actionable items that you can put into practice on Monday morning at 8 am at your medical school, that will transform the culture of your medical school. It won’t require funding, it won’t require having a committee meeting. You won’t need to get approval from anyone. I’m going to give you the sneaky, kind of secret, stealthy method of basically revolutionizing your medical school, and you don’t need approval from anyone. How does that sound?
I’m so confident that we can come out with this (that you will leave here inspired with at least 2 actionable items) that I thought last night, “You know what I’m going to tell them? That if you don’t leave here with 2 actionable items, I will refund your money for this conference.” That’s how certain I am that you’re going to leave here with some actionable items. But I need your help, because I can’t afford to refund everyone’s money. What I need you to do, this is my promise to you, and I would like you to promise to me that you will interact with me during this conversation, that you will share your thoughts, your feelings, any epiphanies that come up, because again, this is a group effort. We’re not going to solve the medical student mental health and physician mental health issues by being passive and just sitting in our chairs.
I would love to invite you, obviously, to put any distractions away, like Facebook, cell phones, and stuff. I do want you to take maybe some notes, just epiphanies that you have during our time together, a thought that comes up. At any point, I want to invite you to ask me a question. You don’t have to wait until the end, if there’s something that really inspires you or worries you, or a concern you have, just go up to the microphone and ask me a question at any point. I will stop and address your questions.
I have been studying physician mental health now and what makes doctors and medical students happy for 11 years. This is what I love to do. I’m sure you can feel my passion for this topic. I would appreciate for you, if there’s an opportunity to share something with a neighbor, please share from your heart. I’ll tell you, I sometimes get coaching before I do public speaking especially in the TEDMED thing. They made me memorize every word and do it like a Broadway show. I got some advice, some coaching, before I came here to speak to you all. The coaching I got was from a medical student named Jamie (who’s an osteopathic medical student in California). She told me what I need to do is not worry about messing up and just open my heart and speak to you all just like we’re having a one-on-one conversation. That’s what I’m going to do. There’s no PowerPoints. I’m not a PowerPoint person. I’m not going to show you any graphs or charts or anything like that. I’m going to tell you real stories of things that I’ve seen and witnessed and messages that medical students have for you that we would like you to hear.
In order for this to work the best, I need for the first 3 rows to have no empty chairs. Who would like to come up and fill the chairs? Raise your hand if you’re on the first 3 rows, and there’s an empty chair next to you. This is a great opportunity to just grab a seat up here. Thank you. This is the type of topic, again, that we’ll … That I ask for you to get up out of your seat and take a risk and sit close to me. I’m very nice. I don’t bite. The reason why it’s so important to sit towards the front is I have prizes for people in the first 3 rows. You’ll get many more of the prizes. You’ve kind of got to claim your seat in the first 3 rows. There’s about 5 more seats left, please come on over. Thank you. I brought a table of prizes here. I guess they’re more like bribes to try to help people get up out of their chairs and participate. This is going to be fun. Look, there’s 4 more chairs, 5 more chairs. Thank you so much, everyone for working with me. You might get to meet somebody that you haven’t met yet if you just … Two more, one in the front.
How I’d like to start is by celebrating the fact that we already have 6 people in the room who’ve won a prize. You might not know it yet, but you’re going to find out real soon. I’d like everyone to stand up. We’re going to meet the winners and what you’re going to have to do is look under your chair, really far under your chair. There might be something taped under your chair and that’s your prize. The people in the first 3 rows have … Did you find it? You can turn your chair over. Oh look, she got one. I can’t wait. Go ahead and open it. Open it, and let’s see what you’ve got. Open it all the way up. Wow, what a … Just tear it open, and the winners I need you to come up to the front. What’d you get? She got a $100 bill and a Starbuck’s card. All right, come on up. I told you, it was really worth coming up to the first 3 rows. Do we have all 6? Everyone, raise your hand with your award, and come on up to the front. Bring it with you. Thank you. I just wanted to meet you, all right, great. $50 bill, Starbuck’s card, all right. Let’s hear it for these people, all right, wonderful. Uh-oh, there’s only 5. Somebody didn’t get one. There’s one left. There’s only 5 people standing up here. Keep looking, keep searching.
The reason why I do that is not … I like to have fun, I think you probably get that from me. I’m a fun person. It’s fun for me to give prizes, but the thing that I do is I feel like people, what it says on there is, “You’re a winner.” I think that’s what I wrote, “I’m a winner,” or “You are a winner”? Everybody should feel like a winner just for showing up. Right? It takes a lot to get up in the morning and come sit in the first 3 rows. I don’t think that we necessarily appreciate people enough for just showing up. This is something that I take into my office. I have a cute little clinic, where I see patients for 30 to 60 minute visits. I actually have patient appreciation days when every patient gets a balloon and a little prize when they come in. They don’t know it’s going to happen, and they’re so excited because who knew that they were going to get a prize from going to visit their doctor, right? Then I have (as if that’s not enough) a gift basket by the front door of my office, where I have additional prizes for people who’ve lost weight or quit smoking, or if I happen to see in the chart it’s their birthday today, I’m already prepared. I can give them a gift if it’s their anniversary. Sometimes, I get gifts from patients that I don’t really need, like baby clothes. I never had kids, so I put that in a gift basket, because there might be other people that come in with kids, and then I send that along. It kind of circulates the love, and it celebrates people, and it makes people feel special.
I believe everyone needs to feel like they’re a winner. Think of the world we would have if everyone felt like a winner, just for showing up and giving it their best. What would that do for medical student morale?
I want to tell you a little bit more about what medical students feel when they get into medical school. I want to see if I can … Let’s see if you can raise your hand if you are currently a medical student. Raise your hand. We’ve got a whole bunch of them there and a few here. Great! I’m going to come back to you. How many of you used to be a medical student in your life at some point? How many of you have never been to medical school as a medical student, but you hang out at medical schools? All right, so most of you have no idea what it’s like to be a medical student, but you probably sense that it might not be that easy all the time.
I’d like to have 3 medical students raise their hand who, if you can remember … Can you remember what it was like when you got the letter in the mail that said you were accepted to medical school? Can you remember that and how excited you were? I need 3 very excited medical students to come up here and take a seat, and share with us how exciting that was that day when you got into medical school. We’ll just pass this around, and just briefly, what were you doing, and the excitement, the joy?
Jessica: Good morning. My name’s Jessica Palmieri. I’m in my third year at Michigan State. I was on a train. I got an email when I was on a train going to visit my family in Kansas City. I had WiFi for no time, and then I had WiFi for 30 seconds, and that’s when I got the email, and I was really, really excited, and then I was panicked because I was like, “Oh no. I’m going to be a doctor and that’s a huge responsibility.” That was my second thought.
Pamela: If you could just complete this thought: Why were you so excited? Did you have some sort of a dream? Or did you see some sort of a destiny that was now possible for you because you got that text or email or however they’re telling people these days?
Jessica: I’m going to be a pediatrician, maybe in the NICU, and I’ve wanted to do that since I was really little. When I was 5, I had this little journal, and I did these little squiggles, and then I had like equals cancer (like cures for cancer) and then I had it for like AIDS. I was 5. I wanted to be a physician for my whole life, and then when I finally got that email . . .
Pamela: It made your dreams come true! Wow. Let’s hear it for her. That’s beautiful.
Female student: I’m [inaudible] (please email me if you know this woman’s name), I’m a third-year medical student at Alabama College of Osteopathic Medicine. I’m sorry I had to go after Jessica, and I’m sorry you have to listen. When I first realized that I was going to go to medical school, I actually got a phone call from the dean of students, and I was asleep. Class got cancelled, you know how that goes. My phone rang and normally I don’t answer my phone, but I looked down and I answered my phone. They said, “Hi, how are you, congratulations, you’ve been accepted.” I got the phone call, which was followed up by an email. I’m not a morning person at all, but I was wired after that. I was so excited. I just couldn’t believe it was all happening.
Pamela: What was your dream? What did this make possible for you?
Female: Kind of like Jessica, I wanted to be a physician since I was little. I was actually inspired by my rural, small-town family medicine doctor. The first day I came in he said, “She’s going to be a doctor, right?” “Yeah, I can do that.” I was a rambunctious child. I was going to be a ballerina, astronaut or a doctor or a lawyer. I was like, “I’m going to be a doctor.” I’ve wanted to be a doctor ever since I was 8 years old, and just to get that call to say, “Hey, now what you’ve been wanting to do since you were a child is finally coming true.” It was awesome.
Pamela: Beautiful.
Stephanie: Hi, I’m Stephanie and I’m a third year at Marshall University School of Medicine, but I’m actually taking a break. When I got my letter, I had just finished working out in the gym, and I almost did a flip on the wall in the locker room. I was so excited. I started texting and calling everybody (and of course everyone’s at work so no one’s available). That was wonderful. It was a stepping … It was seeing the pieces coming together, and achieving your dream. I also wanted to be a ballerina too, but I passed 5’6” and I realized that dream was never going to come true.
Pamela: What is your dream in medicine? What was the dream that came when you got that letter you said, right? What did that make possible for you?
Stephanie: An email, sorry.
Pamela: An email, sorry, yeah.
Stephanie: It meant that I could start my journey. I could start. I wanted to be an orthopedic surgeon. I love that field, and it meant I could start.
Pamela: All right, let’s hear it for our wonderful medical students. You get a prize. You can pick whatever you want. How about that? Look, we’ve got Pet Goats & Pap Smears books, very good. We’ve got physician … We’ve got little stickers, we’ve got little bags with … By the way, in the bags, and in many of the gifts, there are seeds for produce. You may wonder, what does this have to do with growing a doctor? I didn’t originally get this, until I put these bags together this morning. I was like, “Oh wow, good metaphor.” I hand out seeds to my patients during … Instead of just saying, “Eat more fruits and vegetables,” I hand them a packet of seeds and give them instructions on how to grow it, even if it’s on their balcony of their apartment building. I think it’s nice to show people, instead of just tell people. Whatever you like, there’s Starbuck’s cards and stuff in there. You can get more than that, if you want something else. There you go, all right.
I have to admit, I absolutely love medical students.
I think they’re the coolest people in the world, especially right before they get into medical school, and maybe like the first week of medical school. They’re like awesome. They’re so alive. Their dreams are on fire. Come on, you’ve all seen it, right? The reason why I love medical students is because I think they make me a better version of myself. You have these … They’re like these super-curious humanitarian sponges, right? They just follow you around, and they want to know everything you know. Is that cool or what? Your own kids could care less, right, but medical students follow you around. They want to know everything from why you ordered that lab test which makes you wonder, “Why did I order that lab test?” They want to know every little detail and it’s just super cool, because some of us our spouses don’t even take that much interest in us.
It’s kind of cool to have somebody be really interested in your every move, and everything that you’re ordering and why with your patients. That makes me, because emotions are kind of infectious, because they’re so curious, it makes me more curious about what I’m doing. Who’s had that feeling, like you’ve got a curious medical student following you around. Does that kind of make you wonder, “What am I doing and why am I doing this?” It’s good, it’s like a safety valve or something. It’s good. Make sure you don’t do anything too stupid.
They’re very inspired, especially early on. They tell you, they want to work at the homeless shelter and start a clinic in the middle of a poor area in Arkansas, and they have all sorts of dreams. It makes you want to do the same thing. I always wanted to work in a homeless shelter and start a clinic for the poor in Arkansas too. You start to reassess, “Am I really doing what I was called to do?” These people are on fire and it’s great to just be around them.
The third thing, and I’m going to go out on a limb here, it’s probably unique to me, although I think the 2 other women that cried yesterday might feel something like this on occasion, so when I’m with medical students and residents, and it was super cool, the first time I felt this was with this gentleman here. Can you stand up and maybe tell people. This guy started my whole speaking career. I can’t even believe I’m seeing him again, so maybe. Hi. Do you want to tell people who you are?
Dr. Richard Terry: They know who I am.
Pamela: They know? OK.
Richard: Richard Terry from AACOM.
Pamela: You took a risk on me back in, what, 2005? It was kind of risky.
Richard: I read an article you wrote and I just cold-called you and said, “Come do grand rounds for us,” and you came across the country and did it. I can’t remember the topic exactly.
Pamela: It was “Create Your Ideal Medical Clinic.” Yeah. Thank you for that.
Richard: Thank you.
Pamela: This is something that I felt the first time when I was speaking to his group. I never told him this. I don’t need 2 mics, although I have a big message, and I want more people to hear it. This is a little odd. If it’s TMI, just cover your ears. When I’m speaking to medical students and residents, I have this weird feeling like I’m breastfeeding. I know it sounds really strange, and I have never had kids, and I don’t even know what breastfeeding feels like, and half the room doesn’t know either. It’s like, I don’t know, it’s like this love, nurturing energy. It felt like they were all baby birds, just sitting there like this. I don’t know how to explain it, but it was like I kind of felt high after that experience with his group of people there in upstate New York.
Richard: I don’t know if it was mutual like that.
Pamela: It’s just, I never had kids, so I don’t know, maybe … By choice, because it looks like it’s hard. There’s a lot of work to do when they’re young. I like them when they’re already talking, and they can ask you intelligent questions and you can have conversations, not just sit there and need stuff from you. Anyway, that’s why I love medical students.
Pamela: Now, a really interesting thing started happening when I started hanging out with medical students, is that I started getting fan mail from medical students. Like, he told me after I left that there were lines of people lining up at his office trying to figure out how to get in touch with me, how were they going to do the same thing. It just was cool. I got letters … I never got fan mail in my life from anyone else, but medical students. I got fan mail, and then I started feeling like they were asking me advice, and then I felt like I was running like a “Dear Abby” column for medical students. Then, I started getting all my Facebook friends are like medical students, my entire social circle has turned into medical students.
Then a few months ago I got this Facebook message. I’m going to read it to you, because it really impacted me. December 3rd, 2015: “Dear Dr. Wible, I’m not sure you read your Facebook messages, but feel compelled to thank you. I was finishing term 2 of med school and had a bottle of Xanax in my hand. I was ready, as so many of us are. I took 3 and then 3 more. I came across this link, ‘How to Graduate Medical School Without Killing Yourself,’ which I believe may have saved my life, and a couple of close friends who were also suffering. I’m near the top of my class, and praying for death to escape the trap I’m locked into. I was in true delirium from lack of sleep and fear of failure, studying in my sleep and waking up every hour in panic. Med school is doable, but why must it be taught in this format? I read your stories, and I’m just in shock, how many others feel like I do, or I feel like they do. Please keep sharing. You’re saving lives, friend.”
The back story on this is that I did a lecture in Lebanon, Oregon. I wasn’t invited by the school to do the lecture. I was invited by the medical students. There’s all these medical students who keep throwing … I feel like I have to keep throwing these life rafts constantly out to medical students. They’re begging me to come. The administrators haven’t invited me to the schools, but I’m really glad to be here, thank you. It’s one of the reasons I’m glad to be here, but the medical students keep inviting me, and I keep going and speaking for free, because they’re medical students. I don’t want them to have to go and like sell brownies door-to-door or whatever. They don’t have any extra money, so I go. It’s only an hour from my house. It’s a new school in Lebanon, Oregon. I spoke there. I did this talk, and I take all my talks and I put them online, because I feel like more people can benefit from them, than just the people who live down the street from me. This particular one got a lot of interest, like people were reading this a lot. I could tell on Facebook that there was just extreme interest in this topic. What I did is I’ve spent over $3,000 on Facebook ads to promote this lecture that I gave in Oregon, to a targeted audience of medical students to try to stop them from killing themselves. It looks like it was effective. I don’t know how many other people read this and were impacted the same way, but I’m really happy that I was able to save this gentleman and 2 of his classmates, but I feel like there’s got to be a better method than me sitting in Oregon, putting money on Facebook ads. There’s probably a better way to do this, but still, that’s one way that works.
Let’s see here … I kind of want to know, if you don’t mind, now that I have this out, what your reaction is to this. When I read this, did you have a reaction of some sort, some sort of thought or feeling? What I want you to do is just for maybe 5 or 10 seconds, just feel or think whatever that is, and I want you to turn to your neighbor, and I’d like you to just share what that feeling or thought is, that you had when I read this. Just take a minute and share, if you don’t mind. [crosstalk] If there’s some of you who don’t have a partner, you can keep sharing. Some of you might be sitting there because you’re in between 2 people that are talking on either side of you. Come on up here, I’m going to give you a chance to share with me. I need 3 people who are willing to come up and share some thoughts that you have. [crosstalk] I need 2 more brave people that are willing to share. This is a topic that won’t heal itself. This is one of those things where you have to get up and do something about this. Yeah, you can have more. I just want to give a big shout-out to Sharon, because she already won a prize, and she’s up here again, and that’s great. Go ahead, maybe introduce yourself and share what . . .
Dr. Craig Lenz: Hi, my name’s Craig Lenz, and I’m the dean of the Alabama College of Osteopathic Medicine.
Female in audience: We love you, Craig, you know that.
Craig: I was the dean in California from ’99 to ’03, and it made me think about. There was a student that killed himself while I was dean, and I know we had a lot of people that wondered what could be done. Honestly, my background in emergency medicine is that I’ve kind of come to the conclusion that when people get in a deep, dark place, there’s nothing you can do to help them. At the same time, I’ve wondered if there is. It’s probably more on the prevention side of changing the culture, if we can do it. There’s so many pressures that students have, and pressures to pass boards and pressures on loans. When you said that, I just thought back to him. You feel pretty helpless when that happens.
Pamela: Thank you. Let’s hear it for him for getting up here.
Dr. Sarah Parrott: Hi, I’m Sarah Parrott and I’m in the division of primary care at Kansas City University. When I heard you read that statement it made me think about the students who are doing well, but not doing well enough in their own eyes. They come to my office and they close the door. I keep candy in my office so they can always say, “I’m going to Dr. Parrott’s office for candy,” and then they shut the door and start crying. They talk to me about how getting an 85 on a test (which beats the mean) is not good enough because they were an A student in undergrad, and they need to be getting high As so that they can match into whatever specialty. When we were talking about it, my colleague from medical school went to Des Moines University and graduated in 2002, and Sharon Thompson is here. She’s sitting next to me, and she wrote down, “They feel any failure is fatal.” I don’t know how we can get past that, but that’s exactly what I was trying to put into words that she wrote down. I told her, “Go up and say that,” and she’s like, “No, you do it.” I’ll give Sharon my prize.
Pamela: Okay, thank you.
Sharon: We have a similar situation because Tim and I were talking and he said, “I wonder why they feel trapped? What does that mean?” I said, “I’ll tell you exactly what it means.” A lot of students that I interact with as well (and I’m Sharon O’Malley from ATSU SOMA in Mesa, Arizona). One student came to mind really quickly, and he felt very trapped because he was third year, had so many loans that there were not many other jobs that would be able to pay that loan back, so that’s one trap, and then the family let-down of not being a physician and graduating is the other trap. This student was really contemplating not finishing, and wanted to leave and said his mother wouldn’t talk to him for 3 months because he wasn’t going to be a doctor. His wife was really planning to leave as well if he didn’t fulfill his goal for the family. He was always meant to be the doctor in the family since he was a little kid. He actually ended up being treated for clinical depression and he’s back doing a great job.
Pamela: Great. Let’s hear it for our brave physicians who can pick a prize. If you’d like to have another one, you can. I know it’s hard to get up in front of a group and to share something that’s emotional, but this is the exact territory we need to go into so that we can prevent these suicides. I want to share what happens, that’s even more difficult than sharing, although you’re very brave and courageous to have done this, by the way. Even more difficult, I think, than sharing, getting out of your seat here in Washington, D.C., at the Renaissance Hotel, is when you have to talk to the parents and tell them that their child died at your medical school. That’s really, really tough. I want to introduce you to 2 parents, who this month will be the one-year anniversary of having lost their beautiful son 10 days before he was supposed to graduate from A.T. Still there in Kirksville, Missouri. We can go ahead and play this clip, where you can see them. Dim the lights.
VIEW NEW MOVIE TRAILER: (old version transcribed below)
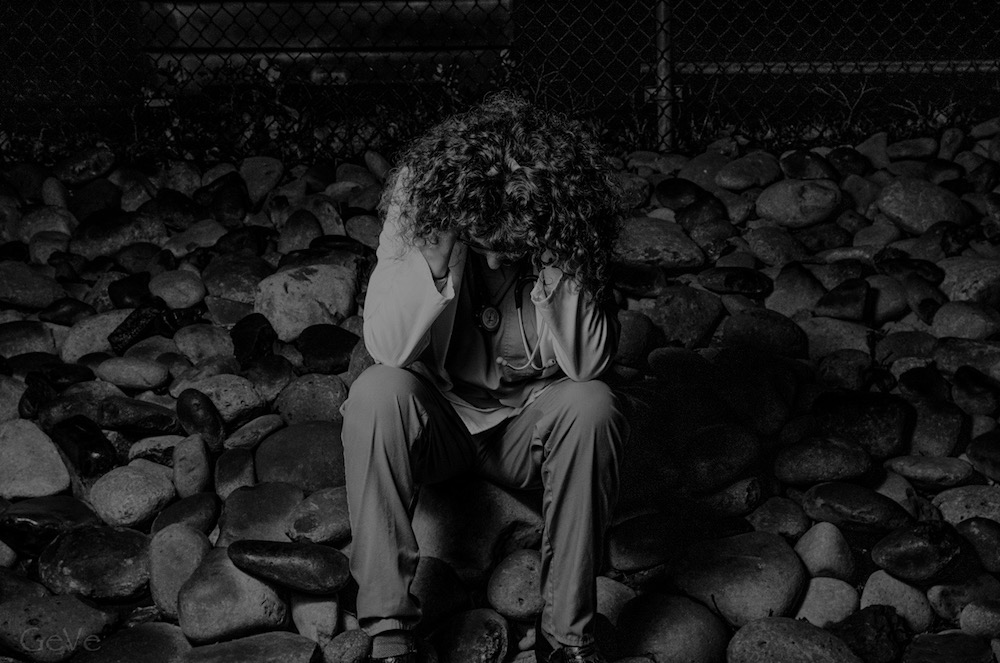
John Dietl: As soon as I lifted the garage door up, I smelled the fumes so my assumption was asphyxiation. I really couldn’t see into the car. I could just see his hand on his leg. He had taken precautions to put something over his head so that we wouldn’t see him.
Pamela Wible: Jumping off the hospital rooftops. Medical students that are found dead in the libraries at medical schools. Their suicides were like well-planned school projects. They’re straight-A students. They’re perfectionists. They’re very good at suicide and they know how to do it.
Hawkins Mecham: Knowing the anatomy, I knew that if you cut yourself on these arteries that you could bleed out pretty quick if you hit them.
Greg Mims: I took a more than fatal dose of benzodiazepine because my plan was to shut down 3 or 4 body systems. I had thought this through.
Kim Perry: There’s a lot of ways that physicians can get controlled substances and narcotics and abuse them.
Rhonda Elkins: Getting ready to graduate valedictorian.
Pamela Wible: Kaitlyn, she was like the perfect little girl. As a third-year medical student she overdosed by helium.
Greg Mims: I left a note in my pocket that read save me if you think I’m worth it.
Pamela Wible: It’s like an extreme cry for help in a profession that’s wounded. If we had this number of patients jumping from hospital rooftops there would be an investigation in this country. Why are we not taking this seriously when these are doctors and medical students?
Keith Frederick: If a third of them are suffering from clinical depression and at risk for suicide or poor quality of life that should be known. That should be exposed.
Female student: Take a couple of deep breaths for me . . .
Kim Perry: The biggest risk is patient safety and quality of care. If you have somebody that is not functional either mentally or physically, then you can’t have good quality of care.
John Dietl: We were so proud and so ready to think about all the great things that this young man could do. He was tremendous. He was my best friend. We said when this very first happened we are not ashamed and we’re going to do anything we can to keep others from having to go through this because let me tell you, it’s hard.
Michele Dietl: I’m very angry that this has been such an issue for so many years. It’s the dirty little secret that nobody wants to talk about.
PLEASE SUPPORT THIS FILM. We have an urgent need for donors to complete the project. Donate here: Do No Harm
Pamela: You can turn that off now. Before you think about this for too long, I want you to turn to your neighbor and just share what it is that you think you could be doing to prevent the next death, the next Kevin. What could you be doing now? The answer is not “Give the national suicide hotline.” The answer is not “Go see Jenny in the counseling office.” I’m asking you what you could personally do to stop this next suicide. If you can’t think of anything then maybe you can get help from your neighbor. Just take a minute to share what you personally think you could be doing. [crosstalk] I would encourage you to continue this conversation, which is obviously more than a 1 or 2 minute conversation. I would encourage you to continue to think about this, and to talk about this amongst yourselves, in your free time between sessions and such. I have 2 people that would like to share some information about what they’re doing, and what they personally feel like they can do to stop these suicides.
Maureen: Hi, I’m Maureen McAteer. I’m a third year student at Marian University College of Osteopathic Medicine, in Indianapolis. I have been honored to be on a task force this year called the Mental Health Awareness Task Force as part of the osteopathic mission to try to figure out a solution to this growing problem. As part of the task force this year we decided to study where we stand as osteopathic medical students. One of the items that we asked everybody in the survey was suicidal ideation. I’m honored to have Nate Prechak (someone correct me if I misspelled his name) who’s helping me on this project, talk about that.
Nate: When Dr. Wible had shared the letter she got about suicidal ideation, we can kind of jumped up and ran up here because in our study (which we’re going to be presenting on tomorrow) we measured a whole slew of different challenges and one of them was suicidal ideation. Of those who took our study, over 1,000 students had marked that they had suicidal ideation.
Pamela: Which was what percentage?
Nate: It was 10 percent of the respondents in our survey, which is over 1,000 students. We felt that that was so important to share because it’s not isolated cases that Dr. Wible had just read about. We found we were shocked that that is how common it is.
Maureen: I think it’s . . .We’re going to talk about it a lot tomorrow at, what time is our talk, 8?
Nate: I think so.
Maureen: We’re going to talk a lot about what we found and it’s extremely interesting where we stand. The most important part is the solutions and that’s I think where we all come in. I think part of the solution is something that this physician this theme (hit on earlier) is this is a cultural shift that needs to occur. I think one of the things we need to focus on is shifting the culture from not accepting help or reaching out for help but encouraging students that it’s okay to reach out for help.
Nate: Something going along with this question, that we can all do is, we can just … Something we should not do, is that we should never make it seem like we should not be seeking help. Any sort of subtle comments you might make that’s what might stick with students. We encourage the comments like that to stop, so students do feel safe to reach out for resources when they need it.
Pamela: Wonderful, all right, get a gift. I want to share what I’m doing to stop this. I’ve now received hundreds of letters from suicidal physicians and medical students, so many that I was able to do a 13-minute TEDMED talk just filled with reading letters. I’ve gotten so many letters that I have a book called Physician Suicide Letters. I wish I didn’t have to write a book called Physician Suicide Letters, but I have so many letters that I don’t know what to do with them anymore so now I’m writing books. Just to let you know, this is a very uplifting book. You wouldn’t think that because of the title, but there’s 53 chapters. 6 of the people have died, 3 are their actual suicide notes published. The rest of them are people who are actively engaged with the idea of should they or shouldn’t they? This is my response to letters that I’ve received back and forth. It’s almost like a book form of a physician suicide hotline because that’s another thing that’s happened as a result of me taking an interest in this topic, at a time when not very many other people have taken interest in this topic … I went to 9 marketing conferences last year, by the way, trying to figure out, “How do you reach guys?” (because it’s mostly men that are dying, by the way). My informal analysis of like 263 cases that have come to me, for every one female we lose 7 men. This is just my data, but that’s a lot. We still have a profession that’s skewed towards men (like 2/3 of practicing physicians are male) but still, for every one female to lose 7 men, how am I going to reach them, or how are they. How am I going to entice them to call me? Should I wear a different color shirt? What should I do? Should I wear less glitter? I don’t know, but I’m trying to figure it out. So I went to these marketing conferences. It’s so funny because they’re like … They ask the audience about competitors and it’s like, “Well, if you don’t have any competitors, raise your hand.” I don’t have any competitors. Nobody is competing with me on this topic. I would like to maybe have more people do something, but essentially this is why I end up doing this hotline.
I have people calling me and emailing me, and sending letters from all over the world, not just the United States. This is a global phenomenon. There’s 8 doctors that we lost in just my town, 3 within a year and a half. I live in a town of 150,000 people. I lost both the men I dated in med school to suicide, not during medical school, but to open the alumni magazine soon after graduation and see my anatomy partner’s name on the obituary, it just really sucks. I also couldn’t find out for years why he died, because of course, the family won’t talk about it. Years later, I found out it was an accidental overdose, and so was the other guy I dated in medical school, accidental overdose. Doctors don’t die by accidental overdose because we dose drugs for a living. That makes no sense. Let’s start telling the truth. If we didn’t tell the truth about ebola or HIV and just hid the bodies, where would we be? Let’s just tell the truth and the truth is that I’ve been going to a lot of funerals.
I went to this funeral for a woman named Rhonda, a beautiful woman who was just incredible. I was standing there. I had many conversations with her before she died. I’m standing there with her whole family, in a rural town in North Carolina, with my hand on her casket, kind of having my final conversation with her. It’s very surreal, because here’s her casket, and then the mound of dirt, and how they put the little fake carpet thing down, whatever, how they set it all up. Over here is like the headstone for Kaitlyn Elkins, her daughter, who was a third-year medical student, who died by suicide. It was her voice you heard on there saying, “Kaitlyn’s going to graduate as valedictorian.” Rhonda couldn’t deal with the grief of losing her star daughter, and so she died by suicide. I’m at a double suicide funeral that also . . . The thing is, this is such a sweet family. They are not vengeful. They don’t want to sue the medical school, although gosh, I might want to, if I lost half of my family to medical school. The thing is, they’re a sweet, nice family. I asked the husband Allyn, I spent the whole day with the grandparents and everyone, the aunts and uncles, and I’m sitting with Alan Elkins, who now lost his wife of 33 years and his daughter. I asked him, “If your daughter worked at WalMart, do you think she and your wife would still be alive?” This guy is like the sweetest guy who would never blame anyone for anything, and he said, “Medical school has cost me half my family.”
This is a serious problem, and it’s not just people that are dying. We’re putting people out into the world who have PTSD. We’re graduating them every year, and they might as well kind of be halfway dead. They’re not all the way there, right? We lose 400 physicians per year to suicide, and that’s not including … That’s like the size of an entire medical school, that we lose every year to suicide. What about the medical students? I don’t even know the numbers there. Somebody told me 75 a year, I read somewhere else 150. Why aren’t we tracking these? You certainly know, when they’re not paying tuition, that something happened, right? They were here last year, and they paid tuition, and here, now they’re not here. What happened to them?
It’s not like … We’re up in everyone else’s business about whether they have guns in their home, and they’re wearing seatbelts, and what their cholesterol is. Then, you lose somebody in your medical school class, and you act like it never happened, or you lose a doctor who jumps off the hospital. It’s very bloody on the sidewalk and we pretend like that just didn’t happen, but then we want to make sure all the patients are wearing their seatbelts and all this other stuff.
This is very strange. Let’s start talking about what we’re going to do about our own people. You almost lost me to suicide. I was suicidal for 6 weeks, and I was normal before medical school. I’m not really normal, but I was the normal me before medical school. In my first year of medical school. I cry easily, obviously. I cried through the meditation yesterday. I cry when movies aren’t even that sad, because I’m just a feeling, emotional person. Let me tell you, I cried so much during my first year of medical school that my eyes sealed shut and I couldn’t even see. I had to feel my way to the bathroom. Why did I cry so much? I was seeing such barbaric behavior. I was seeing things that were just like … I felt like I went back in time 300 years into some sort of a dark age. It was very strange. I could do the work. The academics were not the problem. Just like this guy said, the academics were not the problem. It’s this culture where like we’re 300 years ago.
Actually, we are, because medical education is based on a 17th century philosophy of reductionism, Rene Descartes, right? That’s what we’re basing our whole Western medical education and Western medical system on, where reductionism … We’re just a really interesting bag of skin with a bunch of organs and isn’t it cool how all this stuff works? We’re very micro, micro. It’s really … We’re so micro we’ve lost touch with our hearts and souls. That’s where osteopathic medicine can shine, by the way, since you have on all your websites that you’re holistic, so just let’s do it, right? That’s one of the questions I want you to think about as you mill around for the next few days. Why are we still running our medical schools in 2016 off of a 17th century philosophy? Does that make any sense? Could that be why it feels like we’re in the dark ages?
I think I’ll just kind of rush through this a bit. My story is that I cried my eyes out in medical school. My mom and my dad, who are both physicians, of course I called them on the phone, and they were of no help. They were totally useless to me. I don’t know why they couldn’t help me. Maybe because they were traumatized too and they’re not in their bodies, and so they didn’t have the resources. What was pulled out of them they could not give back to me. My mom sent me Trazodone in the mail. That’s how we handled it. She sent me an antidepressants in the mail, because of course I was probably scared to go to anyone and so my mom sent me psych drugs in the mail which then I took and I didn’t realize how quickly you fall asleep on that, and I almost fell down the stairs and broke my leg.
This treatment for having this major depression due to seeing barbaric behavior among human beings when you thought you were going to medical school is not like an SSRI. That’s not the treatment for abuse. The treatment for abuse is not ADHD meds, it’s not SSRIs, it’s not Trazodone. The treatment for abuse is to say, “Oh, I think he might be getting abused. Let’s stop it. Let’s not do bullying and hazing anymore. Let’s call this what it is.”
And like meditation. I don’t want to hurt anyone’s feelings. I’m Jewish so in a way I can say this, I guess, but if you taught meditation at Auschwitz it’s not going to help that much. They’re still getting abused. We’ve got to figure out, where is this coming from? To run around in circles with little things, which are cool to do, but it’s not going to solve it. It’s like giving somebody who is hypoxic oxygen, but you didn’t treat their pneumonia and they died, because their oxygen is going lower and lower. Let’s just get to the root of the problem, which is I think there’s things we’re doing in medical schools that are not quite right. I’ll leave it at that.
By the way, then what happened is I went to … My mom and I went to the same medical school. She wanted to go back to her 50th year reunion, which was my 22nd year reunion. I didn’t really want to go, but my mom didn’t want to go by herself, and it was kind of cool for a mother/daughter duo to go back to their homecoming reunion at the medical school. Driving there, on the way there, we both felt sick, like we were going to throw up. We almost had to stop on the side of the road. Why is that? I don’t know, PTSD? I don’t know like we’re going back to the scene of the crime, where we felt really bad 50 and 22 years ago, and it’s still affecting us. Can you believe that’s what we’re doing to people? That’s really tragic, that we’re holding this pain in that we experienced. Think about that for a while. It’s kind of overwhelming.
Residency, by the way, was very good. I went to a great residency, and I loved it. I chose a very humane residency that focused on behavioral health and not procedures. Family medicine. I loved it. Then, what made me suicidal … I was not suicidal in medical school, I was just extremely depressed. I couldn’t stop crying for most of first year. By the way, it got progressively better, and third year and fourth year were great, when I could finally get out from … I won’t go into everything that I saw first year that was disturbing to me.
I became suicidal after 6 jobs in 10 years. I was looking for my job. Now that I put all this energy in and I did 24 years of school without stop, kindergarten through the end of residency, and I was ready to finally be the doctor I’d always dreamed of and the only jobs available were factory work. I was at a Toyota manufacturing plant. If I wanted to do factory work and be an assembly-line worker, I would have just worked in an automobile plant, which apparently … In my hospital, by the way, there’s a whole section on Toyota manufacturing in the medical library which is like … They’re actually … I’m not just making this up. They’re running hospitals like Toyota manufacturing plants. That’s why it feels like I’m at Toyota, but that’s nothing that I had originally signed up for.
What I did is this really cool thing, and now we’re in the solutions. This really cool thing that I did is I went and asked my community. I didn’t know what to do. I looked around. Doctors were miserable. I looked at the patients. The patients are grumpy, because they’re not getting care that they need. I was like, “Nobody’s happy. Let me just ask the patients what they want, and let me put the end user in charge. Let me say, ‘I’ll do whatever you want as long as it’s legal, basically, just tell me what you want.” I had 9 town hall meetings over 6 weeks, collected this 100 pages of testimony, which I carried around with me forever. I slept with this. I read this at least 500 times. This became my Bible. This is my life plan. This is the community mandate. This is what people want and guess what? I was able to adopt 90% of what they wanted, and opened one month later with no external funding. Isn’t that amazing? I’m not rich.
It’s just really cool when you put … Hint, hint, hint … The end user in charge, maybe medical students should be in charge of designing their own medical schools, because we don’t always really know what we’re doing, and tradition is just a bad idea held by a lot of people for a really long time. I learned that from my attending in residency. Anyway, why don’t we with fresh eyes, young eyes, people in their 20s who are so excited about life, why don’t we put them in charge and ask them what they want? I started the process by interviewing 500 … I sent a survey out to 500 medical students before I came here. I asked them … I asked 500 medical students, “What are 3 things you’d like to tell your dean but are afraid to say? I’ll do it for you.” Raise your hand if you’re a dean of a medical school. Sorry to put you on the spot here, but here’s what I got back from Sam.
Sam told me … He was one of the first responses, and I thought it was really good, so I thought I’d share that one in its entirety, and then do kind of a synthesis of all the other ones. Sam says:
1) Medical school is the single most unhealthy thing I have ever done for my body, mind and spirit.
2) I was on zero psychiatric medications, and now I’m on more than one, and it’s my second year of medical school.
3) The only communication the administration has with us is through fear-mongering, and the upperclassmen just tell us to get through it. It’ll be over soon.”
That’s how a certain percentage of medical students must feel. It’s probably not just Sam. I have what I kind of wrote as the 10 commandments, the stuff that would be really cool to do, that’s not hard to do. Some of this stuff is pretty easy. You could do it on Monday morning at 8 o’clock, and just start doing what these medical students are asking us to do:
The 10 Commandments for Medical Educators
1) Teach leadership transformation and empowerment in the curriculum. Empower me, so I can empower my patients.” That makes sense.
2) Stop creating an environment that encourages competition among students.
3) Tell me it’s okay to cry in front of patients if it’s on their behalf.
4) Ask what inspires me and ask how you can help me achieve my goals.
5) Respect us as adult learners. Avoid condescension. Don’t revel in our ignorance. We want to learn. Try not to kill our creativity.
6) Advocate for humane treatment of attendings. So many doctors have Stockholm Syndrome and see themselves as strong and capable, while seeing med students as whiny, lazy kids who need to grow thicker skin. They need to be cared for and educated so that they see themselves as survivors of abuse and empowered to break the cycle of abuse.
7) Be more concerned about your students’ wellbeing than damn step 1 scores.
8) Provide emotional support for doctors and med students. Our wellbeing benefits the whole system. We are not the enemies here.
9) Please don’t train me to forsake my humanity to be a better doctor. My humanity should be celebrated, enhanced and matured, not demeaned, degraded or insulted.
10) Show me empathy.
I just got that pretty quickly from a bunch of students that I sent out an email to. I think you guys have access to way more students than I have. You could probably get them. You could do a town hall meeting at your medical school. Here’s a lightbulb idea, and you could ask the medical students to design their own medical school. You don’t have to do everything they say, but wouldn’t it be cool to read what they would write, if they could design their own medical school? Maybe they’d have some really good ideas, and maybe you could employ them right away, right?

I want to just talk a little bit more about solutions. We’ve known that we have a high physician suicide rate since 1858 in England. That’s when I think it was first reported in the literature. Now, we’re 158 years later, and what have we done? Have we made much progress in this? I don’t think we’ve made very much progress. Every so often, there’s a newspaper article, and then it gets buried, or we show a chart and a graph, “Isn’t that interesting at a distance?” and then it gets buried.
What are we doing? We should be doing more, right? What are the solutions? Let me just start with the reaction that you have when you lose a medical student. I want to compare this to school shootings. Since 1980, we’ve lost 320 people in the United States to school shootings. That’s less than one year of the number of doctors and medical students that we’re losing. Look what they do for school shootings. They shut down the school. They let everyone go home. They put flowers on the doorstep of the school. They put teddy bears in the fence. They call in counselors from all over the place to come and help their students. They go to a local church and everyone’s holding candles. They’re on national TV and people are crying and hugging. We don’t do anything for medical students.
Isn’t that a shame? I think it’s so sad, that we just … We’re up their butt on what their step 1 score is and doctors are scrutinized for if they spend one more minute in a room with a patient … I know doctors now have leg timers on like they’re in jail, that time the time they’re in the rooms. We are managing doctors like inmates in prison and the minute they die it’s like they never existed. “You know who that is? I never heard of them.” I just want us to focus on, why don’t we, here’s an idea, handle suicide deaths with the same honoring that we do when we lose somebody at a school for a school shooting? Why don’t we do that? That’s something to think about, instead of hiding it.
Here’s some really good solutions, at the end. You can ask medical students at your school for solutions. I’m sure they are overflowing with ideas on how things can improve. Look at the amazing work that Maureen McAteer. They’re already working on this, right? I would encourage you to ask them.
Here are 3 things that I think you should do. First of all, you can contact me whenever you want. I do want to let you know, IdealMedicalCare.org, contact me whenever. We’re probably not going to have time for Q&A. I thought I had until 9:30, and then they said until 9:15, but anyway, I want you to know that I will be, afterwards, if you don’t get a chance to ask your question, I will be in that Congressional Room B over there, and I will just hang out as long as it takes, and answer anyone’s questions on anything. I’m very committed to nobody leaving here with a question unanswered.
You’re welcome to hang out with me, and even come to my hotel room. I will hang out. I’m staying here the whole time until Saturday morning. You could just … I’m the one with the red hair. You can see me coming. Just grab me, and I am happy to talk about this, because the cool thing is, I think you guys want to talk about this. I’m almost losing my relationship with my partner because all I’ve talked about for 3 ½ years is physician suicide. He’s like, “This is really driving me nuts.”
People are calling me up, like patients, and they’re really worried about me because all my Facebook posts are on suicide. People are worried, “Is something going to happen to me?” I can assure you I’m fine, but I love this topic and I’m an obsessive-compulsive personality, and I won’t be able to get off it until we solve it. I’m hoping that you’ll help me, because otherwise, this could turn into what I do for the rest of my life, and I might want to move on to something else, I don’t know. I had other hobbies, and stuff I do before this. I covered my whole bathroom with mosaics … I saw a bumper sticker that said, “There’s a fine line between a hobby and a mental illness.” Every time I go in that bathroom with the little tiny tiles and the huge scene that looks like you’re on LSD I’m like, “Yeah, I might have a mental illness,” but that’s okay.
Another thing I think we should do, if we lose anyone to suicide, is do a psychological autopsy, or an M&M conference. If you have a suspicious death with a patient, then you all get together and try to figure out, “What could we have done differently?” Why don’t we do that when we lose a medical student, like have everyone … It could be healing. You could call in a counselor, it could be facilitated. We could try to figure out how to prevent the next one, that sort of thing.
Here’s the 2 or 3 easy things that you can do, so I don’t have to refund your money for the conference. One is that when you go back to medical school, whether you’re a student or an administrator, I would just love for you to start using the word “love.” “We love our students,” not just say it, not just put a tag line on your website, “We love our students,” but really open your heart and love your students.
I have these amazing gifts. Who’s an administrator here? I don’t think I gave a gift yet to administrators. I need 3 administrators to come up to the front. I have these really cool gifts, especially for administrators. Here you go.
Dr. Timothy Kowalski: I’ll take one.
Pamela: I want to explain what this is. These are … I went to the Dollar Store, really cheap. I got this book called “413 variety pack stickers.” They say things like, “Great job,” “Wow,” “You’re number 1.” Please reward the medical students in your life. You have 413 options for one dollar, and you could stick this on their little name tags when they come by. You could say, “You know, you’re doing a really good job today” and put that on their name tag. You’ll make their day, you know what I mean? Just simple stuff it doesn’t cost very much. I want you to love your medical students, as much as I love your medical students. Maybe, you’ll start to feel like you’re breastfeeding them or something. It’s a really interesting feeling, but if you start … I know we’re not supposed to use like “love” and “hope” and fluffy emotional words in Western medicine, but just try using “love” a little bit more. When you see a medical student just start thinking, “I love that you’re here at our school, and you’re a winner.” Everyone’s a winner, right? We want everyone to be a winner.
The other thing I want you to do is, why don’t you start thinking of your campus of your medical school as like a family. They’re going to all be there for 4 years with you. Would you treat your relatives like this? Maybe. Would you treat the relatives that you like? You want to treat them like your favorite grandmother and your favorite niece and nephew. These are just people. They’re just like me and you. They cry by themselves at night and nobody’s helping them. It’s so sad. I want you to have like a family atmosphere. It would be really cool the first day of medical school if you welcome everyone and say, “Welcome to the family. You’ve jumped through enough hoops to get here. We are here to support you and we love our medical …” Maybe you don’t want to say … I tell my patients, “I love you” all the time, but some people, boundaries. I heard that an OB/GYN had to go to special boundary classes because a patient gave him balloons. If you feel nervous being a man and telling a woman who’s not your wife, “I love you,” then maybe say, “We love you. We love our students,” and then just show the love. One way that you can all show the love, that’ll really help me get less calls on my suicide hotline, which I never wanted to start, and by the way, I have no suicide training. I never got trained in suicide, so I don’t even know what I’m doing, but these people keep saying I saved their lives, so I’m going to believe them, because they wrote me so they’re still here.
I’m just saying, anyone can do this. It takes no training. It’s just a matter of caring, and opening your heart to somebody, and listening to them, and just being available. I would like you all to go home, and start giving out your home and cell phone number to everyone at your school. Let them know, anytime, midnight, whatever, “You call me. I am here for you. You don’t have to call Dr. Wible in Oregon, although she’s there too, and you could do that, but I’m right here in the same city with you. You call me, and I’ll take you out for tea, or we’ll go sit and you can talk to me on this bench under this tree. I am here for you, and I’m going to do what it takes to make my …” This is what I want you to say, “To make my medical school feel like home, to make everyone at my medical school feel like a winner, and to open my heart to people.” It’s OK. It’s 2016. We don’t have to function like we’re in the 17th century anymore. I think that’s about it, but I’ll take questions. There’s more prizes here, and we’re out of time? We have 5 minutes for questions?

Dr. Donald Sefcik: Sure.
Pamela: Five minutes for questions, and to take the last few prizes. Who wants to ask a question? I’m sure there’s somebody that might be thinking something. Yes?
Dr. Shafik Dharamsi: Do I need to go to the mic?
Pamela: Come over here, yes, for a minute, sure, or just ask here or whatever.
Shafik: This is also more a comment. I’m sure some of you have read Michel Foucault’s “Medical Gaze.” What we tend to do, when we get all of our curriculum and our teaching, is we look out there and we don’t look at ourselves. That’s where the hidden curriculum is. So many of the things that you talked about today, perhaps reflect a hidden curriculum. On the one hand, we want compassionate, empathetic teacher physicians. On the other hand, the way we do things is perhaps antithetical to that, because the way we teach is to look out there before we look within. That’s just a comment. You can respond if you like.
Pamela: I think the answer to this obsession with data and stuff out there is to go into your heart and soul and to connect with each other at a heart and soul level. It’s really cool, all the … We can do lung transplants, and we can do all these things that we can do, but if we’ve lost our humanity, what’s the point anymore? All right, hurry, I have all these books. Any more questions? Yes, come. All right, this is going to be a massive book giveaway here. Questions? What’s your question?
Dr. Diane Karius: My question is, I see a lot of people, sort of the backlash against the trigger warnings and things like that. On Facebook, I’ll see something posted with a trigger warning, “If you’re sensitive to this issue, don’t look at it.” Then, I see a lot of backlash, “You’re not tough enough, you’re not …” How do I fight that message with the students who see that if they say anything, they’re not tough enough? They’re seeing it from a lot of different sources, not just the medical school source.
Pamela: What do you think is the right thing to do?
Diane: I know it’s the way I act and the way … My response is to hopefully be aware of the fact that they are in a place where that’s an issue, but I’m scared that I’m not seeing all of it. I’m not sure. My response, on my own personal level, is I’m disturbed by the “How dare you jump on someone else’s feelings?”
Pamela: I think honesty is always the best policy, honesty and kindness. I, when I first started talking about this, got a lot of backlash from a few older male doctors who were like, “You’re blowing this all out of proportion, shut up. We don’t want to talk about this.” I got reminded about media guidelines for talking about suicide, which apparently I break all of them, to the point where … It’s like, we talk about rape, we talk about everything else, let’s talk about the truth here. My mom is a psychiatrist. Every day, I would go to her house, because she lived in town for a while although she hated Eugene and moved back to Houston. I would ask her, the first thing she said, I’d go in her house, she’d be like, “Have there been any copycat suicides today?” People were accusing me, that I’m causing these suicides now by talking about it. It’s just like, I don’t know where this stuff comes from. One or two more questions, and a quick book here and then I’ll … I want you guys all to follow me to that other room, where we’re going to have a private party.
Female: I have a question.
Pamela: Oh, a question, right.
Female: I don’t know if it’s written here, you were saying if … When we were talking about memorializing the students who do end up going ahead with suicide, if there are students who are on the edge, and they feel like they’re not seen by their administration, or they’re being bullied or whatever, and we put out the teddy bears and the flowers, I don’t know, but will that make people who are on the edge say, “I want them to remember me like they remember Joe.” How do we deal with that delicate balance? I’m a student. I don’t have a training either. I think it would be important to make sure that we say the right thing.
Pamela: Yeah, right. This is uncharted territory, and so we have to walk into it. We’re all caring, compassionate people, somewhere very deep in there. I’m sure that together we could figure this out if we just had more information. Right now, we don’t have the data. We don’t have the information. I’m just collecting phone calls. I think the end goal, obviously, is to change the system so that we don’t have any more people that we need to put teddy bears in the fence for, kind of thing. I don’t really have the answer, but I know we can find it together. I think that’s my answer, is together is the way to go. One more thing and then I’m going to leave. I’m so sorry, this poor man wants me to leave.
Male: Just real quick, if we talk about people who tell students, “This is going to get tougher,” could we perhaps focus on bullying? Bullying has a lot more energy behind it, it seems like, than to talk about suicide. If we could reframe the discussion is that a possible way to get more activity behind it get some people behind bullying as a way to try to stop that as opposed to suicide?
Pamela: Right. And everyone is against bullying. It’s like, everyone everywhere knows that bullying is wrong. Whatever you feel gravitated to work on, if you want to kind of do a zero tolerance for bullying at your hospital or clinic, and maybe you can go to the Dollar Store, they have a whole section on anti-bullying. Just bring those and pass them out at your hospital, and see whether anyone’s doing bullying. They might not even understand this as bullying behavior, because it hasn’t been brought up to them. I’m going to peacefully step to the side.
Dr. Donald Sefcik: I’d love to give you the opportunity to ask Dr. Wible questions until noon. Unfortunately, it’s my job to try to keep us on schedule. Please engage Dr. Wible’s invitation. I will send anyone to her hotel room. I do have 2 housekeeping things that I was asked to talk about, but before I do that, Dr. Wible, I can’t speak for anybody in the room, but I suggest you put some hold dates throughout the summer for potential orientation lectures.