A few months ago, I got this invitation from the director of graduate medical education:
We have 115 residents and no meaningful wellness program to speak of. My goal is to create not only a resident but also a faculty wellness program. To help jumpstart the endeavor, I would love to showcase your work and efforts. I would like to invite you to speak on physician depression and wellness to our residents and faculty.
I love speaking on physician depression and suicide. Wellness . . . well, not so much. Yet last week I helped jumpstart their endeavor (see fun video). I just refused to call it a “wellness program.” Why? Wellness is the wrong word.
Wellness is defined as the state of being in good health, especially as an actively pursued goal. Here’s the problem: actively pursued sounds like work. Wellness is too controlled, measured, and almost forced upon us. Who’s really excited to join a “wellness committee” this week? Or start a “wellness program” at work? Any volunteers? If you’re not that eager, here’s why: the word wellness is boring, overused, and totally uninspiring. Tack on another uninspiring word like committee or program after wellness and you’ve just killed the last drop of enthusiasm in the room. Weirdly, just saying “wellness program” makes us feel less well.
Yet in medicine we strive for wellness. We work hard to help patients be well. So we order lots of labs and tests and check lots of boxes on the electronic medical record to prove how well everyone is. We measure body mass index and blood pressure. We take Pap smears and search every orifice in the human body with scopes and bright lights. And at the end of your Pap and physical we write in the medical record “well woman exam.” How inspiring is that? Patients don’t seem inspired. Kind of a blah experience overall. But, hey, they’re well! Yep, we’re certifying people as mentally and physically well, yet they’re not real excited to be alive. How does that make any sense?
Weirdly, while we’re helping everyone else achieve “wellness,” physicians and med students have high rates of anxiety, depression, and suicide. So medical organizations are racing to create “wellness programs” as the big new innovative solution. Well that kinda seems like forward momentum. But can a wellness committee really save our doctors? Misery in medicine is at an all-time high. I get phone calls, Facebook messages, emails every day from miserable doctors like this one:
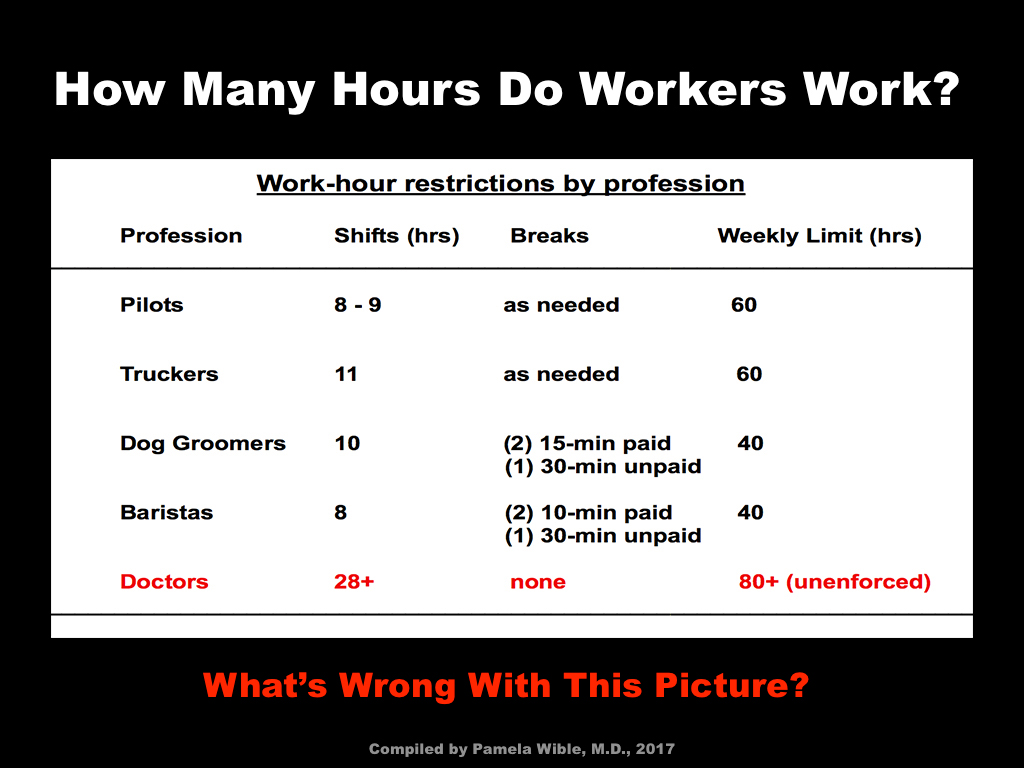
Today I realized that if I become a dog walker and charge $25/hour and walk 5 dogs per day I would make my equivalent salary with a lot less hassles. I’m seriously considering this as a career move. I could be the most over-qualified dog walker out there with a bachelors, masters, doctorate and specialty certification! Sometimes I also dream about becoming a Yogi and Herbalist, maybe a part-time Barista? Maybe that would be more helpful to society than the assembly-line medicine I currently participate in and I would likely be happier and healthier. What do you think?
Here’s what I think. This doctor is well. She’s got normal vital signs. She exercises and eats well. In fact, she’s as well as all the other doctors who tell me they’re dreaming of quitting medicine so they can start organic farms, get certified as yoga instructors, or move to cabins in the woods to write their novels about surviving the trauma of medical training. This is what well-adjusted rational doctors want to do these days. Wellness is not the antidote for misery. Happiness is.

Happiness is a state of well-being and contentment as in joy, delight, even bliss. I’ve never heard of a happiness committee. Maybe because happiness is so untamed. You can’t easily plan for laughter with a committee. Happiness is great and we certainly need more of it, but I’m aiming for something even better—exuberance. Exuberance is the quality of being full of energy, excitement, and cheerfulness. It’s uninhibited and spontaneous exhilaration that’s infectious. Exuberance is happiness on steroids. Physician exuberance is my specialty. Every year, I help hundreds of doctors overcome depression, anxiety, even suicidal thoughts, to become exuberant in medicine.
Oh, when I asked these 115 residents how many felt well, eight people raised their hands. When asked how many felt happy, I got about ten people. What about exuberant? One. Kinda. So I asked how many were sometimes exuberant? Three.

For those who are unfamiliar with the exuberant physician, I’ll share two case studies to demonstrate how to move from blah to exuberance (without a wellness committee stamp of approval).
Case study #1: Dr. Jennifer Zomnir, a family doc in Texas, thought she was living the good life at her 600-doc big-box clinic. Until her husband signed her up for our Live Your Dream Physician Retreat. She didn’t even realize she wasn’t living her dream (she looked about as happy as all the other docs in her clinic). So she arrives at our 150-acre hot springs retreat, has an epiphany that she deserves to live HER dream, quits her assembly-line job and launches her own ideal clinic. Now she works when she wants to, attends all her kids’ events (even takes her children on house calls). She sees all patients over 90 for free! Her patients are over-the-moon thrilled. She’s thrilled. In fact, she’s so ecstatic about her life that she asked me once if she should see a psychiatrist. Why? She’s thought she was manic. Nope. She’s just not used to experiencing exuberance. I recognize her exuberance because I feel the same way in my clinic. Joy and spontaneous exhilaration is our normal state. We should all jump out of bed each day like an excited three-year-old—full of awe and inspiration. That’s normal. Instead, physicians have normalized their unhappy lives so when they’re exceedingly cheerful they think need psychiatric care. Isn’t that weird?
Case study #2: Family doc in New York opens ideal clinic and is so overjoyed that she worries she’ll get arrested. Read her Facebook post:
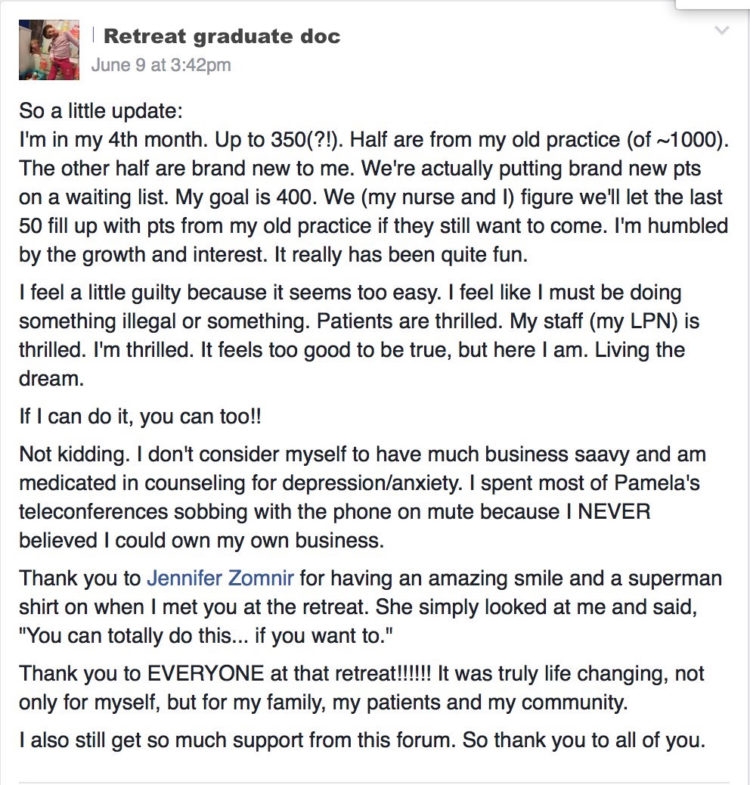
So here’s the weird reason why “wellness programs” won’t work: they’re uninspiring and they mislead us from our real objective: happiness—even exuberance. So how do we get more exuberant doctors and less doctors-turned-dog-walkers? Not by starting a wellness committee. Let’s model what works. Showcase exuberant medical students and residents (there are a few in every program). Bring in exuberant doctors to teach in our medical schools and residences. They’ve already got it figured out.
___
Pamela Wible, M.D., is a family physician and author of Physician Suicide Letters—Answered. View her TEDMED talk Why doctors kill themselves. Ready to live your dream in medicine? Join our upcoming retreat. For retreat scholarships, contact Dr. Wible.