Eleven years ago today I was clueless about doctor suicides. Eleven years ago today at 1 pm I found myself sitting in a memorial service for the third doctor suicide in my town. Eleven years ago today at 3 pm I started asking a very unpopular question that led to extreme isolation, loneliness—even being shunned for asking my question. Although people were whispering in the bathroom about this doctor’s suicide, nobody at the memorial service would say anything aloud. I’m not a whisperer. I like to ask my questions out loud.
I wanted to know WHY doctors were dying by suicide. Not just this doctor. All the doctor suicides in our town.
NOBODY wanted to talk about it.
So I started talking and writing and seeking answers all by myself.
Back then—11 years ago—if you Googled “doctor suicide” you’d not find much. Overnight I was #1 on Google on the secret topic nobody cared to talk about or think about or even contemplate a solution for . . .
Three doctors died by suicide in my town in just over a year. Pediatrician, urologist, cardiologist. Doing the math that means more than 10,000 citizens in a town of 150K had no doctor. When I asked my friend at the newspaper if they planned to cover this startling news, she said “No. We don’t report on suicides unless the family wants it in the obituary.” I explained these suicides were not isolated—that this was a public health emergency. Still the newspaper policy was to censor this news. So I went to the TV station. Spoke to a reporter who took a ton of notes as I shared the loss of our town’s doctors. She called me later to tell me her boss would not allow her to report on our doctor suicides.
I was SO FRUSTRATED!! I asked my therapist how I’d ever get anybody to talk about this and to enact solutions to prevent future suicides. She told me, “You can’t solve a problem nobody knows exists.”
Eleven years later—people are talking about doctor suicide. Many are starting to ask why. A few are ready to hear the truth.
Here’s the truth—idealistic, humanitarian docs who want to do right by their patients are often unable to sustain their passion for helping others in a system that violates the human rights of patients & doctors. Doctors who stand up for patient safety issues (and disturb the money flow) often find their careers destroyed through retaliatory referrals into essentially physician “re-education camps” or “forced drug rehab” programs—even if they’ve never done drugs!
Suicide is not the problem. Secrecy is.
What are the secret shenanigans causing good docs to lose their ability to protect patients from harm?
Let’s talk about money-making scams positioning themselves as “solutions” to doc suicide and organizations that claim to “care for” our distressed doctors while actually putting physician lives at risk—and destroying their careers.
Let’s address REAL issues causing docs to kill themselves.
Today I am grateful. I want to thank everyone for joining me in talking about suicide. I feel less alone. Less desperate because I am no longer the only voice speaking out loud on doctor suicide. Now I’ve even got the DOJ asking questions about doctor suicide!
Here’s a throwback photo to remember the time when I was all alone asking my very, very. very unpopular question.
The widow of one of our suicided docs in town told me, “Keep asking the tough questions.”
Asking the right questions will always lead to the right answers. So here goes . . .
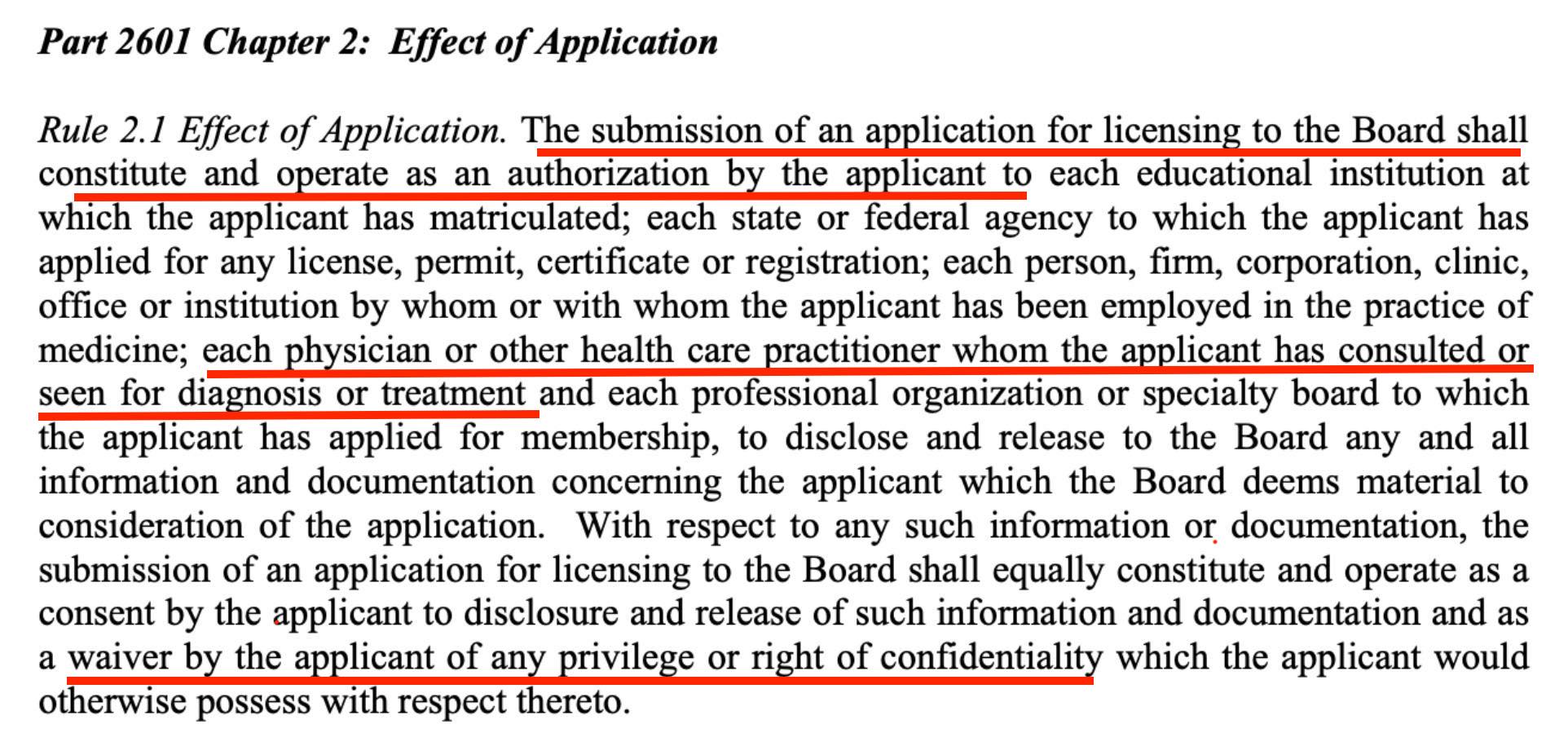
1) Why are so many doctors dying in physician “health” programs (PHPs)? (I personally know 23—tip of the iceberg).
2) Why are competent & qualified physicians forced into PHP evaluations following anonymous, unsubstantiated tips (often retaliatory) with no avenue to explore or appeal allegations of disability or impairment? (good way to get rid of whistleblowers?)
3) Why are physicians with no history of drug/alcohol use automatically enrolled in costly out-of-state inpatient faith-based abstinence programs—followed by five years of drug monitoring and AA attendance?
If we allow good doctors to be driven to suicide—who will be left to care for us?
Just a few questions on my mind today.
Love to know your thoughts.