
Illustration by Jorge Muniz, PA-C. Image credit Medcomic.com
We enter medicine with our hearts and souls on fire ready to serve humanity. By the time we complete medical training many of us have anxiety, PTSD, depression—even suicidal thoughts. Why? Medicine is stressful. Many of us work 100 hour weeks surrounded by suffering and death. We may deliver a stillborn, try to save a teenager with a gunshot wound, and then rush into the next room to help a lady having a heart attack—all within an hour. With no debriefing or emotional support. Medical training glorifies physical and emotional self-neglect and endorses teaching by intimidation and public humiliation. Bullying, hazing, and sleep deprivation is the norm in many of our finest hospitals and clinics. And if we seek psychological support, we’re mandated to report it on all job applications.
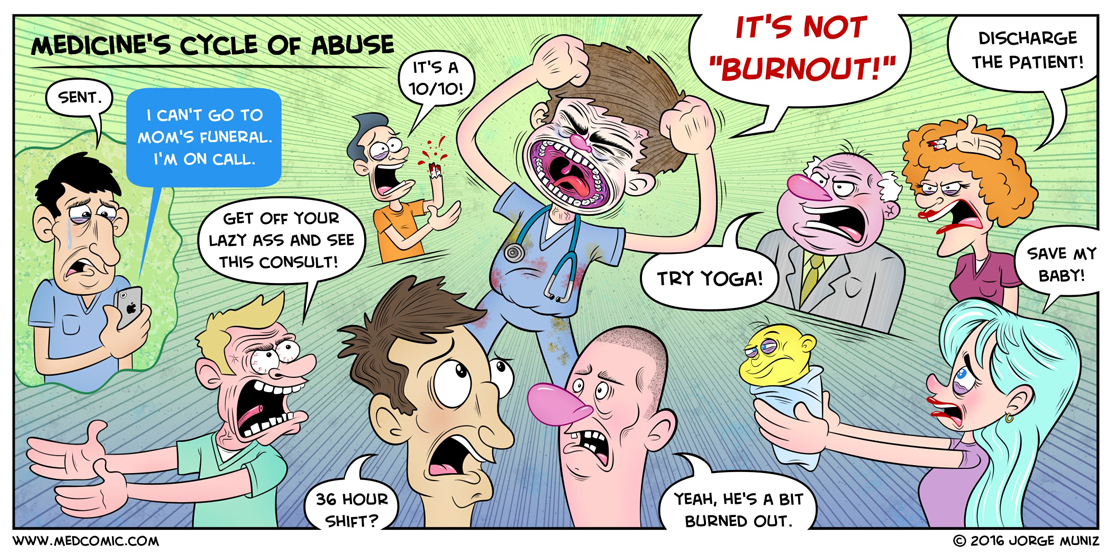
Doctors who complain about inhumane working conditions are often labeled with “burnout,” a “resilience deficiency” or even “disruptive.” They’re mandated to resiliency classes so they can learn mindfulness, deep breathing, or yoga. Victims get instructed in work-life balance, boundaries, and other ways to conform to their workplace abuse.
Anger, grief, and depression are normal responses to a sick medical system that forces us to submit to inhumane working conditions. “Burnout” blames the individual. Physicians may then feel unfit for the profession they once loved. The most vulnerable among us may leave medicine. Some may consider suicide.
“Burnout” and similar labels are dangerous to the individual and also distract from the real diagnosis—human rights abuse. (FYI: Meditation, yoga, and taking deep breaths are not treatments for human rights violations.)
The United Nations Declaration of Human Rights Article 5: No one shall be subjected to torture or to cruel, inhuman or degrading treatment or punishment. Article 24: Everyone has the right to rest and leisure, including reasonable limitation of working hours and periodic holidays with pay.
Doctors, if you on a 36-hour shift in the ICU and have not eaten or pooped all day, you are experiencing multiple human rights violations. Patients, if you’re in the hospital and your doctor is bullied, abused, hypoglycemic, and sleep deprived, you should be very, very concerned. Human rights violations will adversely impact your care.
So docs, how do you know if you’re experiencing human rights violations at work? 1) You don’t get lunch or bathroom breaks. 2) You are forced to work multiple-day shifts. 3) You are not allowed to sleep. 4) You are forced to see unsafe numbers of patients. 5) You can never seem to find “work-life balance.” 6) You are threatened verbally, financially—even physically. 7) You are bullied. 8) And if you ask for help, you’re called a slacker or worse.
If any of this seems familiar, it’s not your fault. You are a victim of abuse. So what should you do? Your goal should not be to cope with abuse. Your goal should be to stop it. Taking deep breaths will not end your abuse. If you’re being abused, speak up. If you’re complicit with abuse, you perpetuate the cycle on the next generation.
Other countries get in big trouble for human rights abuse. Why should US health care get a pass?
Here’s what happens when we are complicit with medicine’s human rights violations:
Pamela Wible, M.D., advocates for a humane medical education system and is an activist in medical student and physician suicide prevention. She is author of Physician Suicide Letters—Answered. Contact Dr. Wible here. Jorge Muniz, PA-C, is an internal medicine physician assistant, illustrator, and author of Medcomic: The Most Entertaining Way to Study Medicine. Image credit: Medcomic.com.














Retired OB writes: “So flipping true!!!! (Long long long pause as I just stare out into nothing with phone in hand remembering so many of those times)”
Another doc: “This is straight out of the Soviet era. Better to be labeled ‘resistant’ than ‘sick.’ #InvertYourFlags”
I Definitely think I love you
This is a brilliant distinction that you have made.
Thank you
Hi Pam, scripe57 (Steve Cripe RN) from Twitter. We don’t often agree on this issue. But for the sake of NOT having an arguement, let’s call it a human rights violation, not burnout. Great article, but you’ve taken us all right up to the point of….
What do we do about it? You’ve educated us on what you believe it really is and you feel that by calling it “burnout”, we blame the victim. Who says? If we label some handicapped, we don’t blame them. if we say a person is diabetic, we don’t blame them. Why do you feel we blame the victim of burnout? And again, what do we do about it? What’s the answer? Do we all call the ACLU or hire lawyers and sue the hospitals? I know, lots of questions…but there aren’t many answers I’ve read about. Just asking…
When we use the word disabled or handicapped we address this by making systems accessible to the handicapped (elevators, ramps, wheelchairs etc . . ). We do not tell the disabled to adjust to a building or system that does not work for them. And the ADA helps prevent discrimination by outside organizations, employers, etc. . .
It is the intention—how “burnout”is being used to deflect responsibility from the system and pile more on the to-do lists of the victims. “Take meditation, yoga, and a class on work-life balance” instead of the system taking this on and reducing work week hours to avoid sleep deprivation, having zero tolerance for bullying and intimidation in hospitals and med schools (this has been done in elementary schools so can’t be that hard to follow their lead). It’s not difficult to solve this problem once we say it out loud and recognize it for what it truly is.
Follow the medical SOAP note model. Make the correct assessment/diagnosis: Human rights violations. Then create a plan. Simple.
I’ve outlined the solutions for years on my blog. For example here are 2 articles detailing simple nearly cost-free solutions:
https://www.idealmedicalcare.org/blog/medical-student-suicide-simple-solutions/
https://www.idealmedicalcare.org/blog/humanizing-medical-education-how-to-grow-a-happy-doctor/
Funny thing is Steve, I had been primarily focusing on solutions (with little traction) and then my friend pointed out: “Ya know Pamela, you can’t solve a problem nobody knows exists.” So my focus is now increasing public awareness and decreasing professional denial. We are our own worst enemies in medicine.
Don’t recognize that you’re a victim, then you are at high risk of becoming the victimizer. And the cycle continues.
#1 is Eliminate the word “burnout” from the lexicon: Not only does burnout minimize the severity of depression, detachment and (at extremis) suicidal ideation among healthcare professionals (HCPs), it implies that those suffering post-trauma have some inherent flaw or weakness that impairs their ability to remain functional. This mindset removes the onus from the system.
Having been married to a doctor, the mother of a doctor and a nurse, and daughter and sister of nurses, I have long thought the treatment of medical personnel is abusive and completely uncalled for. There is no excuse for these long shifts and verbal abuses piled on top of good and loving people who give so generously to the wellbeing of us all. It is long past time to change these paradigms!
Amazing. Thank you!!
My “leadership coach” tried to convince me I need to meditate. It’s true. But seems to be a much easier fix to put the owness on the physician instead of the broken system.
They tried to tell me that in residency too. Told me I needed to see a psychologist. Again, it was an abusive system. Me seeing a psychologist (who could not possibly understand) fixed nothing.
You always hit the nail on the head with your articles.
Best,
Kari
You hit the nail on the head with this one Dr. Wible!
Hi Pamela,
I just read this piece and I realized that I might be in the ideal place to help some people.
As a trained doctor I have first-hand experience with this situation. That said, I have just received a Masrers’ Degree in Counseling Psychology and I am about to open my own clinical psychology (ideal!!!) practice has a primary care doc. MDs who see me do not have to have the psych piece on their records.
Anyhow, I wanted to throw that out there in order to try and help. I am licensed in Massachusetts so I can care for anyone in the state – in person, or via video.
Hope you are well!
Jill
Congrats to you! You are a unique medical doctor with psychology degree and who is a trained therapist! Was curious, did you pursue residency or did grad degree in Psychology after finishing med school?
I am so blessed I never pursued pre-med and do not have true interest in becoming a physician or nurse though admire what they do. I have usually been more into behavioral sciences and community which is I am pursuing a MA in City Planning. I now I am more into lifestyle and food based medicine and despise medications.
How sad and cruel many children of doctors pursue med school to show something as revenge or as bad being forced or imposed into it when their heart is not in it.
Dear Dr. Wible, So I take from this article about physician/resident abuse, that this is the reason I have been denied pain meds for chronic pain?
Eliminate the word “burnout” from the lexicon: Not only does burnout minimize the severity of depression, detachment and (at extremis) suicidal ideation among healthcare professionals (HCPs), it implies that those suffering post-trauma have some inherent flaw or weakness that impairs their ability to remain functional. This mindset removes the onus from the system.
Sitting on the deck (my equivalent of your tree house) in the growing dawn, reading GRIT by Angela Duckworth. I got to page 258 and found a quote that caused me to jump from the chaise and grab my computer. I had to send this to you asap.
The quote from John Schofield at West Point (1879) which cadets are still required to memorize, “The discipline which makes the soldiers of a free country reliable in battle is not to be gained by harsh or tyrannical treatment. On the contrary, such treatment is far more likely to destroy than make an army.”
She goes on to delineate the great reduction at West Point effected by changing from an attrition model to a developmental model, ceasing to use fear to achieve high standards to “leading from the front,” which is based in “unconditional respect.”
My vision, and I know yours, is transforming medicine from fear to unconditional respect — which is a stones throw from the love I was talking about yesterday.
Love the synchronicity of finding the quote this morning!
Have a fabulous day! Rita
Hi Pamela, I agree, human rights violations are endemic in medicine. People feel they have the right to bully and do not even realise or care that they are bullying. Care and compassion needs to be the heart of medicine, beginning with our doctors and medical students, for only when one lives in and is treated with Care and compassion can one truly be that with another. Our current medical culture is to be blunt disgraceful. Rather than being the bastions of human rights abuse that we currently are we instead ought to be the institution that is the bastion of true human rights, true care and compassion for humanity, something lived by and with all staff as well as patients for we are all equal and all have and ought to have access to the same human rights, decency, respect and care. True human rights are the foundation of true health. Abuse does not lead to health or healthy health care providers.
Thank you so much for your story… I never would have thought some people
who are so young (who was supposedly going to be a doctor) taking her own life
in this thing that is been going on etc.
I have never heard that story before, and I always thought most doctors are happy with theirs
job as it one of the most important role in life. I am really touched by this story.
Thank you
Good article and cartoon. I like the comment in the corner of the cartoon about not going to a funeral. Too much personal sacrifice and too much expected sacrifice for those who work for physicians. I remember when my friend told me that the cardiologist he worked said that my friend couldn’t go to the funeral of his best friend. Because the MD sacrificed, he expected the employee to be willing to sacrifice too.
And the cycle of abuse continues. Please speak up. Silence will not save us. Submitting to cruelty is not the answer.
If some patients would be a little more considerate and not be an ambulance chaser or someone who promotes doctor-shaming through media, this is one way to address the issue
A well noted important distinctions. The term “burnout” inappropriately blames the individual rather than squarely placing the blame on the system.
This is the right thing to do.
This distinction of a problem- individual vs. system is well established in the Medical Errors literature.
Ya Basta con “Burnout”
Please name the doctor who fired her.
Burn Out happens only if one does not like the job or the job does not pay well or some one at the job is abusing you. I loved my job but harassment and discrimination from some nurses was enough to switch the love button to burn out. Previous 2 jobs were harassment from a physician and discrimination when my colleagues did not wish to cover for American African physicians. I refuse dot accept it and decided to leave.
I wish physicians were united and cared for each other truly without selfishness or jealousy. Everyone is so busy in their work and personal lives and so consumed by fear of losing their job or privileges, that one feels lonely. This loneliness is a seed that grows and finally one explodes into depression or outrage. Both are detrimental…
PLEASE STOP USING THE VICTIM-BLAMING WORD “BURNOUT.”I’ve been asked to submit an article for a special edition journal on physician burnout. I wrote back stating: I think it is essential that you frame this conversation in a way that stops blaming the victim. I’ve written extensively on this and welcome you to use any of my previous blogs.
Editor: I totally hear you on victim blaming and explained the question of use of the term burnout on the From the Editor page of the current issue. It’s difficult, though, NOT to use that term when all of the medical organizations do so and it’s the term the public has become accustomed to, so I use it, albeit reluctantly, with an explanation that the term itself is a poor way to describe the issue.
Me: The longer we allow inaccurate and harmful terms to be used against physicians, the longer we will suffer. Just because everyone says it doesn’t mean it’s right. We don’t describe rape victims as sluts. So lets stop blaming doctors with the word “burnout” If we keep using the word burnout its like calling a firefighter to put out fires when 100 arsonists are in the loose. We’re not going to get very far. Stop burning down our physicians with this word. Please.
The TED MED was excellent although tragic. This is something we need to talk about. The way medical students are trained should change. Why does it have to be so brutal? Who in the world would want to go into a career like that?
My son was born with a heart defect. It saddens me to know that there are doctors in our congenital heart defect community who have committed suicide. We families grieve over the loss of our doctors — people who become like family to us. We, as a society, need to make some changes to see that this occurrence lessens.
Thank you for shedding a light on this issue. Maybe now we can start working on some solutions.
I wondering of countries outside the USA have a much better health care system where healing is done through lifestyle and food rather than medicine and doctors from residency onwards have best balanced lifestyle onwards?
I would assume Canada, Nordic Countries, Taiwan, etc right?